










Abortion in the United States 2017: Preliminary Review and a Call for Reform

This is Issue 14 of the American Reports Series.
Originally published on May 22, 2019, and has been updated on July 3, 2019.
Compared to other United States vital statistics reporting systems, the U.S. abortion surveillance system has been consistently recognized as incomplete and out of date. For instance, in November 2018, the National Center for Health Statistics (NCHS) released a report containing final birth data for 2017.1 The report was based on data from every state and the District of Columbia. Similarly, in November 2018, NCHS released a report containing final 2017 mortality data from each state and the District of Columbia.2 In contrast, the most recent abortion surveillance report from the U.S. Centers for Disease Control and Prevention (CDC), which was also published in November 2018, is based on data from 2015 and is missing data from three states. States report abortions to the federal government on a voluntary basis, and California, Maryland, and New Hampshire – which together account for an estimated 20 percent of all abortions performed in the United States – do not report abortion data to the CDC.3
State-level abortion reporting indicates that this delay is unnecessary and may be obscuring identification and interpretation of rapidly developing changes in U.S. abortion trends. The Charlotte Lozier Institute has analyzed data from 37 states that released abortion reports for 2017 by April 2019, more than a year and a half ahead of the CDC’s established timetable (Table 1). Together, these 37 state reports allow for an early peek at U.S. abortion trends at the national level and suggest that, among other developments, the decades-long decline in U.S. abortions may be slowing.
Table 1. States with Published 2017 Abortion Reports (37)
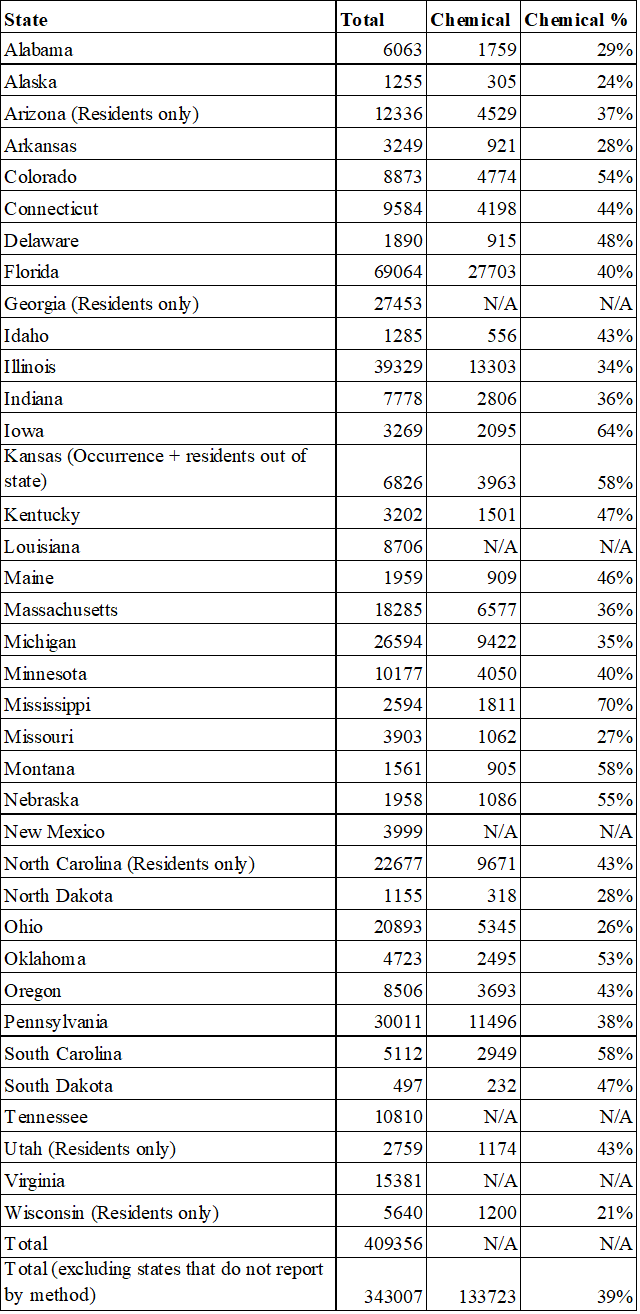
Chemical Abortion
Of the 37 state abortion reports, 32 contain information on the types of procedures used to perform abortions. This includes information on chemical abortions, or abortions that are induced chemically rather than surgically. Most commonly, chemical abortions are induced with a combination of the drugs mifepristone and misoprostol. In 2000, the U.S. Food and Drug Administration (FDA) approved the use of mifepristone (commonly known as RU-486) as an abortifacient for use early in pregnancy. Since then, chemical abortion has become an increasingly frequent method of abortion in the United States. In 2016, the FDA further relaxed some of its restrictions on mifepristone and expanded the stage of pregnancy at which the FDA authorizes its use, subject to a variety of risk mitigation requirements.4
State-level abortion reporting indicates that the revisions to the FDA protocol in 2016 may have had an impact on chemical abortion rates that is not yet reflected in CDC reporting. In 2017, chemical abortions made up 39 percent of abortions reported by the 32 states that specify abortion methods. By contrast, the latest report from the CDC, which is based on data from 2015, estimates that chemical abortions represent just 27 percent of reported abortions.5 The CDC notes that chemical abortions have rapidly increased over the past decade. However, the delay in national abortion reporting means the most recent estimate from the CDC underestimates the true percentage of abortions that are chemically induced and does not reflect the increase in the proportion of chemical abortions after 2016.
This underestimation has ramifications for public health. Chemical abortions have a much higher complication rate than surgical abortions performed at the same point in pregnancy and result in more frequent visits to the emergency room.6, 7 Unfortunately, information on complications resulting from abortion in the United States is very limited. Ohio, one of only a few states to require the reporting of abortion complications, shows that adverse events caused by mifepristone are rising as chemical abortions in the state increase.8 The lack of accurate chemical abortion data at the national level means that adverse events caused by chemically induced abortions may be much more common than researchers realize. Exacerbating the problem, the FDA’s adverse event tracking system now only requires reporting of chemical abortion complications that result in death, allowing the vast majority of complications to go unreported.
Changing Abortion Trends
Additionally, state-level abortion reporting from 2017 suggests that the prevalence of chemical abortion may be impacting the national abortion rate. Abortions in the United States have been falling since the early 1990s. In 2015, the CDC reported 652,639 abortions in the U.S., the lowest number since 1973.9 Consistent with other recent years, this does not include abortions performed in California, Maryland, and New Hampshire. However, state reporting for 2017 indicates that this decline may have begun to level off.
Of the 32 states that reported information on abortion methods for 2017, 25 reported chemical abortion data annually from 2008 to 2017 (Figure 1). Since 2008, total abortions among these 25 states have declined by 23 percent, while chemical abortions have increased by 68 percent. Between 2015 and 2017, total abortions fell by three percent, while chemical abortions rose by almost 20 percent.
Figure 1. States that Reported Chemical Abortions 2008-2017 (25)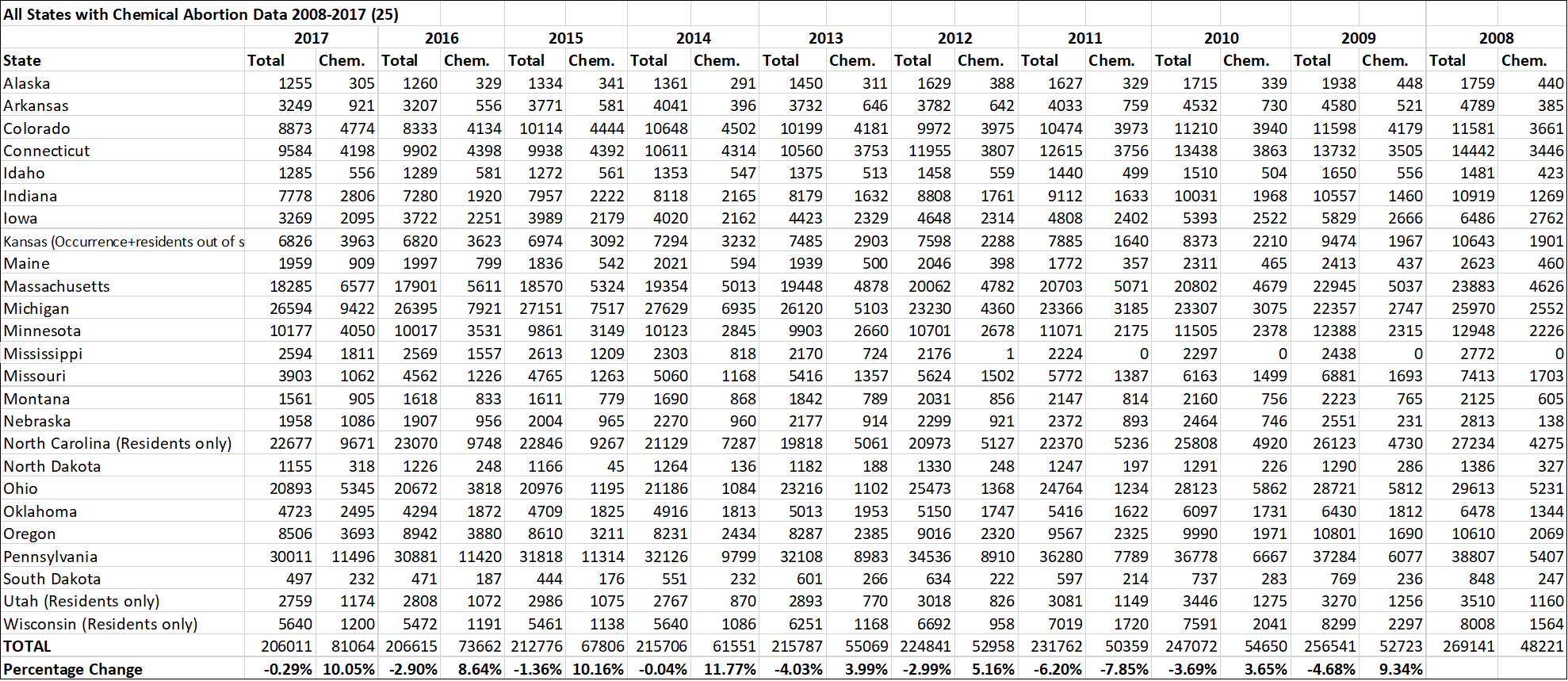
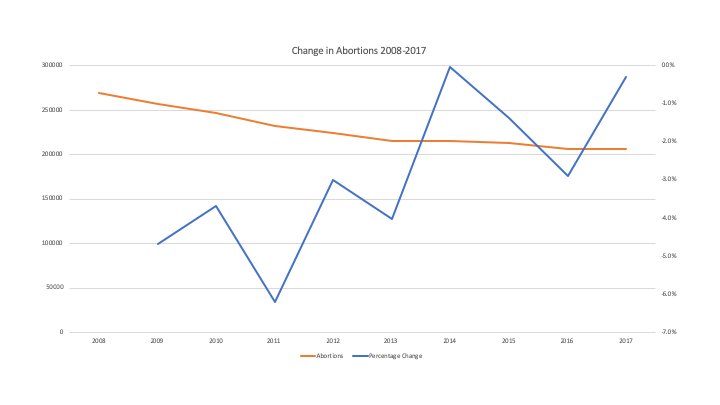
However, the abortion decline may be slowing: total abortions fell by just over a quarter of a percentage point between 2016 and 2017, compared to a drop of almost three percent the previous year (Figure 2). Among these 25 states, abortions declined between 2016 and 2017 by the second-lowest margin in the entire 10-year period.
Figure 2. Change in Abortions Among States that Report Chemical Abortions 2008-2017
This slowing of the decline in total abortions may be attributable to chemical abortions. Among the 30 states that reported total abortions and chemical abortions for both 2016 and 2017, 16 states saw declines in total abortions. In these 16 states, abortions dropped by four percent. Chemical abortions in these 16 states also declined slightly, by one percent. In comparison, 14 states saw increases in total abortions from 2016 to 2017. Overall, abortions among these 14 states increased by two percent from 2016 to 2017, while chemical abortions increased by 21 percent.
Limitations of Abortion Reporting
While the available reported abortion data is useful for analyzing abortion’s impact, it is still difficult to draw comprehensive conclusions about abortion in general in the United States due to delayed, incomplete, and inconsistent abortion reporting. As already noted, the national reporting surveillance system via the CDC lags two years behind other vital statistics systems, namely birth and death data, and misses more than a fifth of all abortions performed in the U.S. Regarding chemical abortions specifically, among the 37 states that have reported data for 2017, only 25 reported chemical abortion data for a full decade. Even among those 25 states, reporting is variable. Some states report abortions performed on residents only, rather than all abortions occurring in the state, for example.
In 2016, the Charlotte Lozier Institute released a study that surveyed abortion reporting across the 50 states and the District of Columbia and ranked the states based on the quality of their reporting.10 States like Oklahoma and Minnesota received the highest scores for collecting a wealth of data and making it available to the general public in comprehensive reports that are released in a timely manner. States like California and Wyoming received the lowest scores for declining to make abortion data publicly available or for failing even to collect it at all. These limitations plague the CDC’s abortion surveillance reports. As CLI pointed out in 2016, there is no single data point for which information is available for all 50 states. The CDC’s data for chemical versus surgical abortions is missing nine states. To help bridge the gap, CLI regularly publishes annual summaries of state-level abortion data, noting key trends and providing recommendations to individual states. However, without a national, mandatory abortion reporting system, U.S. abortion data will continue to be outdated and incomplete. As rapid changes in abortion policy and provision affect the nature and public health implications of abortion in the United States, accurate abortion reporting remains an issue of urgent concern.
Tessa Longbons is a research associate for the Charlotte Lozier Institute.
7/3/19 note: In July 2019, the Minnesota Department of Health revised the 2017 abortion report to reflect the addition of abortion reporting forms that were received after the report had been published and the removal of abortion reporting forms that were incorrectly filed. There were 10,134 abortions in Minnesota in 2017, of which 4,015 were chemical abortions.
References
- Martin, J.A., Hamilton, B.E., Osterman, M.J.K., Driscoll, A.K., & Drake, P. (2018). Births: final data for 2017. National Vital Statistics Reports; Vol. 67 No. 8. Hyattsville, MD: National Center for Health Statistics. Retrieved from https://www.cdc.gov/nchs/data/nvsr/nvsr67/nvsr67_08-508.pdf
- Murphy, S.L., Xu, J.Q., Kochanek, K.D., & Arias, E. (2018). Mortality in the United States, 2017. NCHS Data Brief, No. 328. Hyattsville, MD: National Center for Health Statistics. Retrieved from https://www.cdc.gov/nchs/data/databriefs/db328-h.pdf
- Jatlaoui, T.C., Boutot, M.E., Mandel, M.G., Whiteman, M.K., Ti, A., Petersen, E., & Pazol, K. (2018). Abortion surveillance — United States, 2015. MMWR Surveillance Summaries, 67(No. SS-13), 1–45. DOI: http://dx.doi.org/10.15585/mmwr.ss6713a1External
- S. Food and Drug Administration (2019). Questions and answers on Mifeprex. Retrieved from https://www.fda.gov/drugs/postmarket-drug-safety-information-patients-and-providers/questions-and-answers-mifeprex
- Jatlaoui, T.C., Boutot, M.E., Mandel, M.G., Whiteman, M.K., Ti, A., Petersen, E., & Pazol, K. (2018). Abortion surveillance — United States, 2015. MMWR Surveillance Summaries, 67(No. SS-13), 1–45. DOI: http://dx.doi.org/10.15585/mmwr.ss6713a1External
- Carlsson, I., Breding, K., & Larsson, P.-G. (2018). Complications related to induced abortion: a combined retrospective and longitudinal follow-up study. BMC Women’s Health, 18, 158. Retrieved from https://bmcwomenshealth.biomedcentral.com/articles/10.1186/s12905-018-0645-6
- Upadhyay, U.D., Desai, S., Zlidar, V., Weitz, T.A., Grossman, D., Anderson, P., & Taylor, D. (2015). Incidence of emergency department visits and complications after abortion. Obstetrics & Gynecology, 125(1), 175-183.
- Longbons, T. (2018). Abortion reporting: Ohio (2017). Charlotte Lozier Institute. Retrieved from https://lozierinstitute.org/abortion-reporting-ohio-2017/
- Jatlaoui, T.C., Boutot, M.E., Mandel, M.G., Whiteman, M.K., Ti, A., Petersen, E., & Pazol, K. (2018). Abortion surveillance — United States, 2015. MMWR Surveillance Summaries, 67(No. SS-13), 1–45. DOI: http://dx.doi.org/10.15585/mmwr.ss6713a1External
- Donovan, C.A., & Gonzales, R. (2016). Abortion reporting: toward a better national standard. Charlotte Lozier Institute. Retrieved from https://lozierinstitute.org/abortion-reporting-toward-a-better-national-standard-summary/















