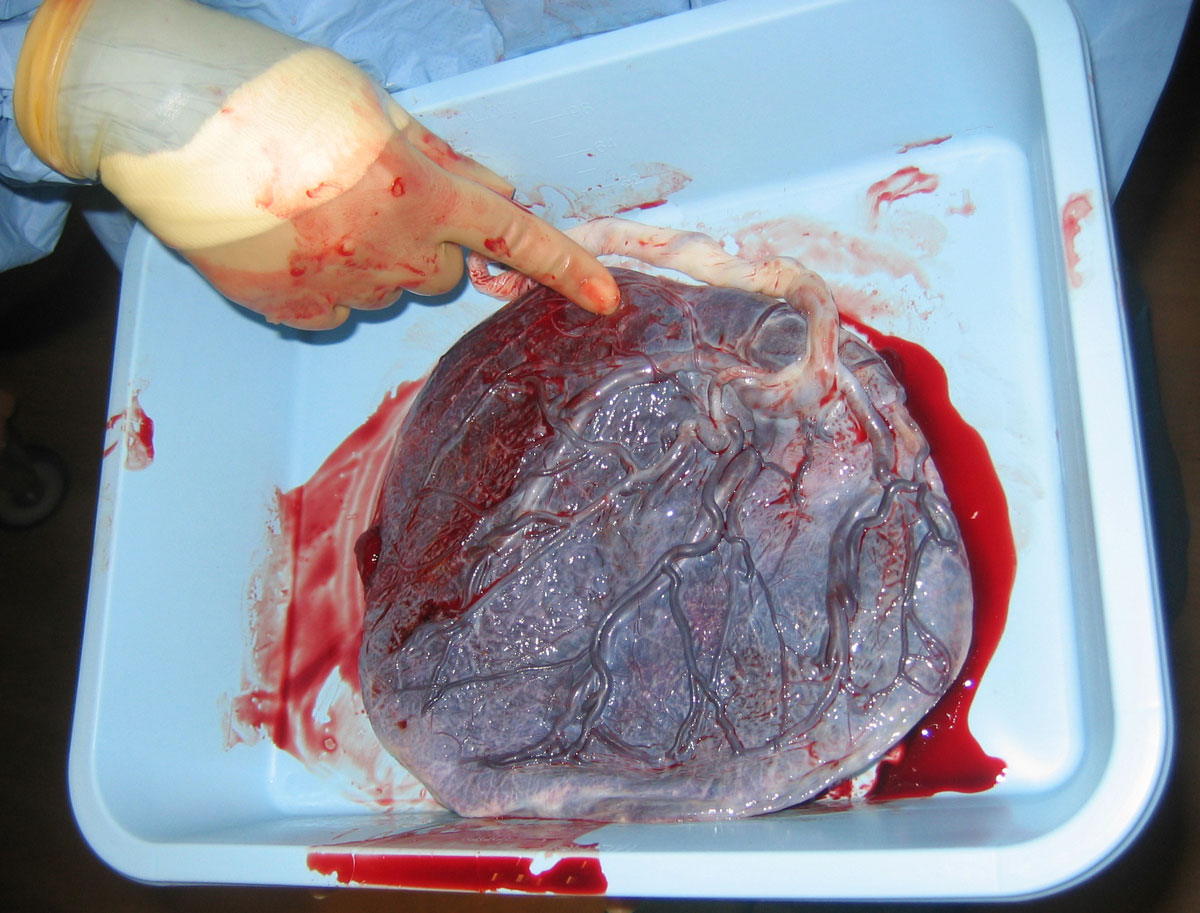
The placenta forms as maternal and embryonic tissues interact. During implantation, the outer cells of the embryo, called trophoblast cells, invade the uterine wall. The fetal part of the placenta, called the chorion, is completely covered with little hairlike projections called villi until week 10. These tiny branches are filled with fetal blood vessels. Their job is to maximize contact for gas and nutrient exchange while keeping maternal and fetal bloodstreams separate. After week 10, most of the chorion becomes smooth, while the sections that directly touch the maternal part of the placenta develops a tree-like network of blood vessels. Blood vessels from the embryo interlace within the mother’s blood in the placenta.2
The transition to placental nutrition is gradual. Before 7 weeks gestation, the embryo absorbs most of its nutrition from the yolk sac and uterine lining while the placenta is still developing.3 By week 7, the placenta and umbilical cord have developed enough to take over the job of delivering oxygen and nutrients to the embryo and carrying away waste.4
Ultrasound studies can reliably detect blood flow in the umbilical cord starting at 7 weeks gestation. This means the embryo’s heart is actively pumping blood through the umbilical cord to the placenta by week 7, enabling gas and nutrient exchange. The blood flow in the umbilical cord steadily increases from weeks 7 to 10.5
Pregnancy is beautifully engineered so that the fetus receives the right amount of oxygen at exactly the right time in development. For example, oxygen levels are lower during the first 12 weeks and then rise significantly around 13 to 16 weeks to support the growing baby.6 Fetal blood is different from maternal blood in two key ways: (1) the blood has more hemoglobin and (2) the hemoglobin is better at carrying oxygen. Before the placenta is mature, the embryo has less oxygen. Quantitatively, fetal blood can carry roughly 40% more oxygen per liter than maternal blood, so the embryo can thrive even in low-oxygen environments.7
The placenta supports and protects the developing fetus in a variety of ways. One of its key roles is hormone production: it synthesizes human chorionic gonadotropin (hCG), progesterone, and estrogen—hormones essential for maintaining pregnancy and supporting fetal growth. Remarkably, male and female fetuses exhibit subtle differences in how their placentas produce and respond to these hormones.8 Beyond its hormonal duties, the placenta also acts as a protective barrier, shielding the fetus from many bacterial and viral infections. However, even with this defense, some pathogens can cross the placental membrane and cause fetal illness. Fortunately, the placenta helps in the transfer of maternal antibodies during the second and third trimesters, providing the fetus with passive immunity to diseases like diphtheria, smallpox, and measles.9 10 11 The placenta is also responsible for regulating the fetal environment by keeping the fetus’s body temperature slightly higher than the mother’s—typically between 100.7 and 102.5 degrees Fahrenheit.12 The placenta’s life-support capabilities are truly remarkable, creating a bond between the mother and child that no technology will be able to replace.