










Lethal Non-Compliance with Washington’s “Death with Dignity Act”

This is Issue 92 in the On Point Series.
Beginning with Oregon in 1997, ten states and the District of Columbia have legalized physician-assisted suicide (PAS) for patients said to have a terminal illness. These laws passed because voters and elected officials were assured that the practice would be hedged about with strict “safeguards” against coercion and abuse. Yet in recent years, organizations drafting and promoting these laws have urged that the safeguards be weakened or eliminated to increase “access” to PAS.
An example is my home state of Washington, which became the second state to legalize PAS in November 2008 through its “Death with Dignity Act” (DWDA). For the last two years, organizations that sponsored the DWDA have promoted legislation under which lethal drugs can be prescribed by non-physicians, the waiting period between first request and provision of the drugs is shortened from 15 days to three (and in some cases to no time at all), and counselors other than psychologists or psychiatrists can assess whether the patient has impaired judgment due to conditions like depression.[1]
That legislation has now been defeated twice in a state where Democrats control both chambers of the legislature. In both years it was approved by the House but stalled in the Senate, failing even to make it out of Senate committee in 2022.
This was due to the efforts of health care professionals, disability rights advocates, and others to point out the proposal’s dangers to vulnerable patients, and to question whether the “safeguards” are truly preventing abuse even as currently written. For example, the state Department of Health’s annual reports show that: A psychological assessment to detect impaired judgment is almost never requested by the prescribing or consulting physician, so is not done; the prescribing physician is almost never present when the drugs are taken, so cannot report on any abuse or coercion (or the patient’s competency) when the actual decision to die is made; and patients diagnosed as having less than six months to live have survived for years.[2]
Now, study of the Department of Health reports indicates a more alarming abuse: In hundreds of cases, physicians have engaged in illegal activity under the pretext of following the DWDA. To understand this, it is necessary to review how the DWDA and its “safeguards” work.
How the Death with Dignity Act Works
For many years Washington, like most states, has recognized aiding another person’s suicide as a crime, regardless of the perpetrator or the health condition of the victim:
RCW 9A.36.060. Promoting a suicide attempt.
- A person is guilty of promoting a suicide attempt when he or she knowingly causes or aids another person to attempt suicide.
- Promoting a suicide attempt is a class C felony.
The maximum penalty for this felony is a $10,000 fine and/or five years in prison. RCW 9A.20.021 (1)(c).
This law was unanimously upheld as constitutional by the U.S. Supreme Court in Washington v. Glucksberg, 117 S. Ct. 2258 (1997). The parties in this case, including the state attorney general, agreed that the law prohibits a physician from assisting the suicide of a terminally ill patient.
Moreover, delivering a controlled substance such as a narcotic to another person is generally a Class C felony. RCW 69.50.401. The drugs used for “death with dignity,” opioids and barbiturates, fall under this law. That law has a limited exception: “A valid prescription or lawful order of a practitioner, in order to be effective in legalizing the possession of controlled substances, must be issued in good faith for a legitimate medical purpose by one authorized to prescribe the use of such controlled substance.” RCW 69.50.308 (h) (emphasis added).
State law further recognizes the felony of “controlled substances homicide” if these drugs cause death when used by the recipient: “A person who unlawfully delivers a controlled substance in violation of RCW 69.50.401(2) (a), (b), or (c) which controlled substance is subsequently used by the person to whom it was delivered, resulting in the death of the user, is guilty of controlled substances homicide.” RCW 69.50.415 (emphasis added).
The key words here are “legitimate medical purpose” and “unlawfully.” The DWDA renders such activity lawful, but only if its requirements are complied with: “Actions taken in accordance with this chapter do not, for any purpose, constitute suicide, assisted suicide, mercy killing, or homicide, under the law. State reports shall not refer to practice under this chapter as “suicide” or “assisted suicide.” RCW 70.245.180 (emphasis added).
The DWDA itself defines penalties for abuses such as altering or forging a patient request for lethal drugs, or coercing a patient to make such a request. It then adds: “The penalties in this chapter do not preclude criminal penalties applicable under other law for conduct that is inconsistent with this chapter.” RCW 70.245.200 (emphasis added).
In short, if a physician prescribes or provides a drug overdose so a patient can take his or her own life, but does not comply with the DWDA’s requirements, the physician’s actions do not fulfill a legitimate medical purpose and are not lawful. That physician can be prosecuted for promoting a suicide attempt or committing a controlled substances homicide.
The DWDA’s Reporting Requirement
The DWDA requires physicians and other involved parties to comply with reporting requirements, including timely submission of their reports to the state Department of Health, in order to exempt themselves from legal liability:
“The department of health shall require any health care provider upon writing a prescription or dispensing medication under this chapter to file a copy of the dispensing record and such other administratively required documentation with the department. All administratively required documentation shall be mailed or otherwise transmitted as allowed by department of health rule to the department no later than thirty calendar days after the writing of a prescription and dispensing of medication under this chapter, except that all documents required to be filed with the department by the prescribing physician after the death of the patient shall be mailed no later than thirty calendar days after the date of death of the patient.” RCW 70.245.150 (1)(b) (emphasis added). Note that in legislative language, “shall” generally means “must.”[3]
The DWDA instructs the Department of Health to adopt rules to help ensure “compliance” with this requirement, and to contact a health care provider who submits “an inadequate or incomplete report” in order to address that problem. Id.
The Department’s implementing regulation reaffirms the mandatory nature of the reporting requirement: “To comply with the act, within thirty calendar days of writing a prescription for medication to end the life of a qualified patient, the attending physician shall send the following completed, signed, and dated documentation by mail to the State Registrar, Center for Health Statistics…” WAC 246-978-020 (emphasis added).
The required documentation includes a copy of the patient’s “written request for medication to end life,” the Attending Physician’s Compliance form, the Consulting Physician’s Compliance form, and the Psychiatric/Psychological Consultant’s Compliance form (if a psychological evaluation was performed at the request of the attending or consulting physician). A pharmacist who dispenses the drugs must also submit a report, identifying the patient and attending physician as well as the drug provided; and the physician must file an After Death Reporting form within 30 days after the patient dies (from any cause).
The Attending Physician’s Compliance form is of critical importance. Among other things it documents that the patient voluntarily requested the lethal medication orally and in writing, with a waiting period allowing time to reconsider the request; that this request was informed, after being counseled on alternatives; that the patient has a terminal illness expected to lead to death within six months; that the patient was referred to a consulting physician to confirm this prognosis; and that the patient does not have “a psychiatric or psychological disorder or depression causing impaired judgment” (or was referred for psychological evaluation if either physician thinks such impairment may exist). RCW 70.245.040. The consulting physician must also confirm these claims in writing. RCW 70.245.050.
Equally important is the patient’s signed request form, witnessed by two persons who testify that the patient is competent and not acting under coercion or undue influence. RCW 70.245.030.
While these requirements may seem strict, it should be noted that the attending physician controls all reported information. Only that physician is authorized to report on what happened, and to select the consulting physician giving a second opinion. Any information that could lead others to identify the physician or patient is excluded from the Department of Health’s annual reports to the public. The attending physician may also sign the patient’s death certificate and is required by the DWDA to list the underlying illness as cause of death, further preventing outside scrutiny. RCW 70.245.040 (2).
The reporting requirement ensures only that the physician claims to have followed the other requirements of the law. In 1999 the Oregon Health Division, commenting candidly on its first annual report, said: “There are several limitations that should be kept in mind when considering these findings…. For that matter, the entire account [by prescribing physicians] could have been a cock-and-bull story. We assume, however, that physicians were their usual careful and accurate selves.”[4]
Widespread Violations of the Law’s Requirements
Washington’s 2019 and 2020 DWDA reports were not released until August 2021 and October 2021, respectively. The 2021 report, though dated “July 15, 2022,” was not released until November 2022. Thus the Department had ample time to contact physicians and to correct or supplement any initial information regarding cases in the given year. The reports state that 299 participants received the lethal medication in 2019, 340 in 2020, and 400 in 2021. At least 291 patients died from the lethal drugs in 2021 — the highest number of cases ever reported by the state, and eight times as many as in 2009, the year the law took effect. Forty-four patients died of other causes, and another 52 died but the Department says it does not know whether this was from ingesting the drugs. This means that at least 44 lethal overdose prescriptions, and potentially as many as 96, were not ingested by the patient and their whereabouts are unknown. The Department does not claim that any patient was referred for a psychological evaluation in these years.
Most disturbing, however, is the admission by these reports that in many cases the legally required forms were never submitted by physicians.
For the 299 participants who received the lethal dose in 2019, missing required documentation includes:
41 written and witnessed requests from patients
39 attending physician compliance forms
45 consulting physician compliance forms
29 pharmacy dispensing forms20 after-death reporting forms
2 death certificates
For the 340 participants who received the lethal dose in 2020, missing required documentation includes:
45 written and witnessed requests from patients
34 attending physician compliance forms
41 consulting physician compliance forms
22 pharmacy dispensing forms
33 after-death reporting forms*
1 death certificate*
(* Of 334 participants who died)
For the 400 participants who received the lethal dose in 2021, missing required documentation includes:
46 written and witnessed requests from patients
35 attending physician compliance forms
47 consulting physician compliance forms
20 pharmacy dispensing forms
39 after-death reporting forms*
0 death certificates*[5]
(* Of 387 participants who died)
The Department of Health’s reports from previous years show that these violations have been occurring since the law took effect in 2009. However, the annual number of cases (and of violations) has dramatically increased, so that about half the cases in which physicians fail to comply with the DWDA have occurred in the past three years. For example, of the 219 missing attending physician compliance forms, 108 are from 2019-2021. The same is true of 132 out of the 264 missing patient requests, and 133 out of the 257 missing consulting physician forms.[6]
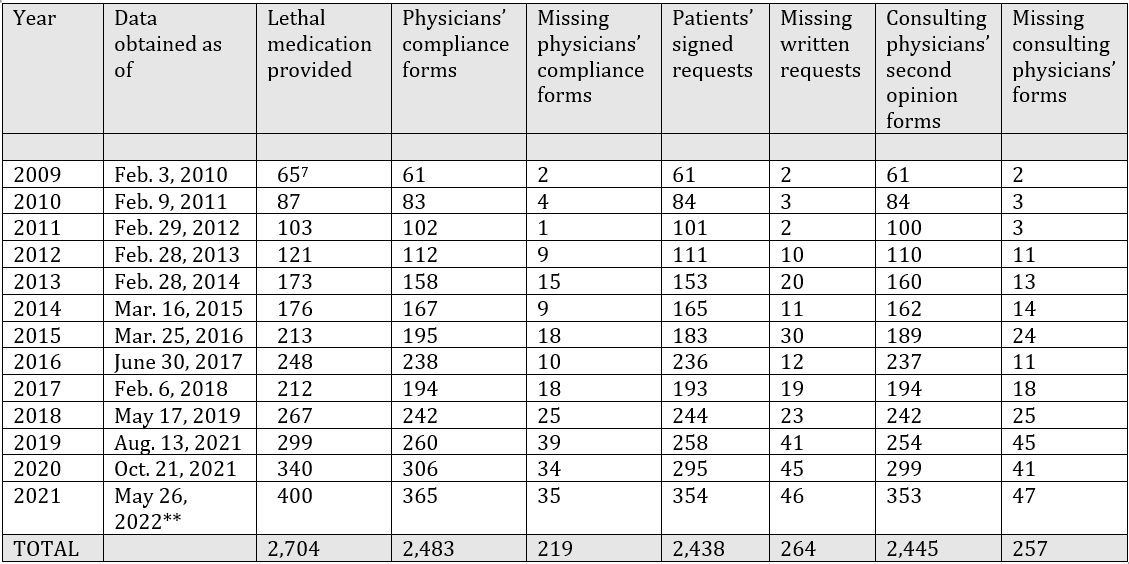
** The 2021 annual report notes that the Department of Health has not yet received all documentation for 2021 participants, although its report on this year did not become publicly available until November 2022.
Table 1. Cases of lethal medication provided “under the terms of” the Death with Dignity Act according to the Department of Health, 2009-2021, and cases in which legally required documentation is missing[8]
Physicians and pharmacists were legally required to submit these forms within 30 days after the events in question, and the Department of Health was legally required to seek out these forms if that deadline was not met. Yet many months (and as long as a year and a half) after these events, in many cases the documentation is missing that would exempt the physicians from underlying criminal statutes, administrative sanctions from the state medical board, and potential civil liability.
In these cases, no one can assume that the person who received the lethal medication had any illness (much less a terminal illness), as no form reporting an illness was submitted; made a competent and uncoerced request; or that the legally required second opinion was ever obtained.
It would be disturbing enough if the missing information suggested that a crime may have occurred – that is, that we simply have no evidence that the lethal drugs were voluntarily requested by a patient in 264 cases, or that the patient was mentally competent and terminally ill in 219 cases. But that would be to understate the case. Providing these reports to the Department is itself a minimum requirement for “compliance” with the Death with Dignity Act — it is the key “safeguard,” a gateway to all others. Without such compliance, criminal and other liability applies. These cases are subject to a felony charge, and do not qualify as “deaths with dignity.”
Yet the Department of Health is not known to have referred any of these health professionals for possible indictment, or for review by the state medical board. On the contrary, it includes these cases as instances where the lethal medication was provided “under the terms of the law.”[9] The report on 2021 cases is especially incoherent on this point. It says that in order to comply with the Act, “attending physicians and pharmacists must file documentation” with the Department of Health. But then it also says: “To receive the immunity protection provided by chapter 70.245 RCW, physicians and pharmacists must make a good faith effort to file required documentation in a complete and timely manner.”[10] As noted above, it is the first statement that is consistent with the DWDA and its implementing regulations.
To be sure, the DWDA does state: “A person shall not be subject to civil or criminal liability or professional disciplinary action for participating in good faith compliance with this chapter.” RCW 70.245.190 (1)(a). But the Act says this does not apply when a person willfully alters or forges a patient’s written request, destroys or conceals a rescission of the request, or exerts undue influence to lead a patient to request the lethal medication – these acts are Class A felonies. It does not exempt any person from civil liability for “negligent conduct or intentional misconduct.” And as noted above, it does not exempt anyone from “criminal penalties applicable under other law for conduct that is inconsistent with this chapter.” RCW 70.245.200.
None of these statutory provisions allow a physician merely to “make a good faith effort” to obey the Act’s explicit requirements. The Act’s references to “good faith” also “do not allow a lower standard of care for health care providers in the state of Washington.” RCW 70.245.190 (4). In fact, the requirement to submit the required reports is so important that the Department of Health is required by the Act to contact the physician to obtain them if they are missing or incomplete — not merely to ask the physician whether the requirement was ignored “in good faith.” Such a standard would evacuate the safeguards of all meaning. RCW 70.245.150.
At the implementation level, then, the “Death with Dignity Act” seems to be a system out of control – or out of the control of everyone except the physicians whose behavior it is supposed to regulate. When the safeguards are not enforced, they become meaningless.
Implications for Efforts to “expand access” to the Death with Dignity Act
Debated but not enacted in recent years, HB 1141 sought to “expand access” to the Death with Dignity Act by weakening or repealing various “safeguards against abuse” that proponents had highlighted in 2008 to win voters’ approval. Groups like Compassion & Choices and End of Life Washington now claim that these “safeguards” are working only too well, to the extent that they are “barriers” to access that must be weakened or eliminated.[11]
The evidence, however, suggests that in practice even the existing safeguards pose no effective barrier to the assisted deaths of people who are not ill and who may not have made a voluntary and uncoerced request. Assistance in causing deaths in such circumstances is a crime under state law.
It may be worth noting that End of Life Washington testified before a state Senate committee in 2021 that it has been directly involved in “95%” of the Death with Dignity cases.[12] Whether that active involvement by an assisted suicide advocacy group, one which opposes the current safeguards, contributed to non-compliance with the Act is not known.
In any event, the state government should be investigating and preventing non-compliance with the voter-approved safeguards, not “expanding” the opportunities for abuse further.
Richard M. Doerflinger, M.A. is an associate scholar with the Charlotte Lozier Institute.
[1] Richard M. Doerflinger, “Assisted Suicide’s Slippery Slope in Action: Washington State May Drop ‘Safeguards’ Against Abuse,” On Point Issue 55 (January 2021), Charlotte Lozier Institute, available at https://lozierinstitute.org/assisted-suicides-slippery-slope-in-action-washington-state-may-drop-safeguards-against-abuse/.
[2] See USCCB Secretariat of Pro-Life Activities, “Assisted Suicide Laws in Oregon and Washington: What Safeguards?” (December 2022), available at https://www.usccb.org/issues-and-action/human-life-and-dignity/assisted-suicide/to-live-each-day/upload/suicideoregonwashingtondec2022final.pdf.
[3] Legal Information Institute (Cornell University Law School), “shall,” citing Nolo’s Plain-English Law Dictionary, available at https://www.law.cornell.edu/wex/shall#:~:text=Shall%20Shall%20is%20an%20imperative%20command%2C%20usually%20indicating,permissive%20provision%2C%20ordinarily%20implying%20some%20degree%20of%20discretion.
[4] Center for Disease Prevention & Epidemiology, Oregon Health Division, CD Reports, March 16, 1999, at 2. Available at, https://www.oregon.gov/oha/PH/DISEASESCONDITIONS/COMMUNICABLEDISEASE/CDSUMMARYNEWSLETTER/Documents/1999/ohd4806.pdf.
[5] The question arises: How did the Department of Health know how many patients received a prescription for lethal medication, if physicians did not submit the forms alleging compliance with the safeguards? These lists provide a partial answer. In some cases a pharmacy dispensing form was submitted by the pharmacist dispensing the drugs; in other cases the physician may have filed an after-death reporting form, or solely a death certificate. None of these forms, however, ask about compliance with the safeguards, although each identifies the prescribing physician.
[6] Figures in the table that follows reflect the discrepancy between each annual report’s figure for number of patients obtaining lethal medication “under the terms of” the DWDA, and that report’s figures for number of various reporting forms submitted: 2009 report, pp. 1, 3; 2010 report, pp. 1, 2; 2011 report, pp. 1, 2; 2012 report, pp. 1, 2; 2013 report, pp. 1, 12; 2014 report, pp, 1, 12; 2015 report, pp. 1, 12; 2016 report, pp. 1, 13; 2017 report, pp. 1, 13; 2018 report, pp. 5, 15; 2019 report, pp. 5, 14; 2020 report, pp. 5, 14; 2021 report, pp. 1, 11. For all annual reports see Washington State Department of Health, Death with Dignity Data, available at https://doh.wa.gov/you-and-your-family/illness-and-disease-z/death-dignity-act/death-dignity-data.
[7] The 2009 report listed 63 patients who had obtained the drugs, but this was corrected the following year when two additional patients were reported (see 2020 report, p. 4). Because the Department did not say whether the required reports by physicians were ever submitted for these two patients, this table uses the original figure of 63 to determine the number of missing reports. This may undercount the number of non-compliant cases, as it may be four instead of two.
[8] The Department of Health does not report how much overlap there is among these instances of non-compliance – whether, for example, most of the 264 missing patient request forms refer to the same patients for which the physician never submitted his or her compliance form. If not, there could be over 700 cases in which one or more of the Act’s requirements was ignored.
[9] In some earlier years the exact phrase used is “under the terms of this law.” One or the other of these phrases is used to describe the total number of lethal prescriptions on the first page of each report that is cited in note 6 above.
[10] 2021 report, pp. 11, 12 (emphases added).
[11] For example, both organizations sponsored the document Bill Summary: Increasing Access to the Death with Dignity Act HB 1141 (2021), available at https://www.compassionandchoices.org/docs/default-source/bill-summaries/wa-hb-1141bill-summary.pdf?sfvrsn=8f7c3def_1.
[12] Testimony of March 17, 2021, before the Senate Health & Long Term Care Committee, watch – TVW, Washington State’s Public Affairs Network, at 49:35.













