Written Testimony of Tara Sander Lee, Ph.D., in Support of Ethical Alternatives to Aborted Fetal Tissue Research

On Thursday, December 13, 2018, the U.S. House of Representatives subcommittee on Healthcare, Benefits, and Administrative Rules and Government Operations for the Committee on Oversight and Government Reform held a hearing on “Exploring Alternatives to Fetal Tissue Research.” The hearing was called as the U.S. Department of Health and Human Services re-evaluates funding for research using tissue from aborted babies. Charlotte Lozier Institute Associate Scholar Tara Sander Lee, Ph.D., submitted the following written testimony in support of using ethical alternatives to aborted fetal tissue research.
To view Sander Lee’s testimony in PDF format, please see, “Written Testimony of Tara Sander Lee, Ph.D., In Support of Ethical Alternatives to Aborted Fetal Tissue Research.”
Written Testimony of Tara Sander Lee, Ph.D.
Associate Scholar, Charlotte Lozier Institute
Subcommittees on Healthcare, Benefits, and Administrative Rules and
Government Operations for the Committee on Oversight and Government Reform
“Exploring Alternatives to Fetal Tissue Research”
December 13, 2018
To the Distinguished Chairs and Honored Members of the Committee:
Thank you for the opportunity to testify before you today regarding alternatives to fetal tissue research. I am a scientist with 20 years’ experience in academic and clinical medicine. My career has focused on the pathologic mechanisms of childhood disease. I earned a PhD in Biochemistry, completed postdoctoral training at Harvard Medical School and Boston Children’s Hospital in molecular and cell biology, and then established my own basic science research lab studying congenital heart disease and vascular disorders in children. Shortly thereafter, I served as Scientific Director of a clinical molecular diagnostics lab. Under my scientific direction, new genetic testing was developed and offered to children suffering with Cystic Fibrosis, 22q Deletion Syndrome, Hearing Loss, blood disorders, and Epilepsy. I have worked with various types of human tissue, including, but not limited to, umbilical cord, heart, skin, blood and post-mortem tissues. I am currently a faculty member, scientific consultant, and Associate Scholar for the Charlotte Lozier Institute. This is my personal opinion on behalf of Charlotte Lozier. I am not representing the views or opinions of any other institution with which I am affiliated.
VACCINES AND TREATMENTS
I stand before you today with a message of hope. We do not need fetal body parts from aborted babies to achieve future scientific and medical advancements. Very little research is actually being done that currently relies on abortion-derived fetal tissues. NIH estimates it provided $103 million for research using human fetal tissue in 2018 of the total NIH budget of nearly $30 billion or 0.36% of the total NIH budget.[1]
This is relatively small compared to billions of dollars funding research that does not involved fetal tissue from abortions. Why? Because several alternatives exist that are abundant, successful, and not tainted by abortion. In addition, science speaks for itself. After over 100 years of research, no therapies have been discovered or developed that require aborted fetal tissue. History has shown us that we never needed fetal tissue.
In the case of vaccines, cells derived from aborted fetal tissue have been used in the development process, but fetal tissues have NEVER been the exclusive means necessary for these breakthroughs. Instead, monkey cells, chicken eggs, and non-fetal human cells are used to produce vaccines for polio, measles, and mumps. The vast majority of scientists are focusing on other ethical tissue sources and models that work just as well, if not better. If we stopped harvesting fresh tissues from aborted fetuses today, it will not stop one person from being treated or vaccinated today nor will it inhibit the development of new vaccines going forward.
Here are the facts:
- Development of the original Polio vaccine was first produced in monkey kidney cells.[2] While historic fetal cell lines (WI-38, MRC-5) were used for the first isolation of the Polio virus and some subsequent formulations have been used, non-fetal alternative formulations ARE currently available in the US. Most polio vaccines currently use the cell line Vero (monkey) in the manufacturing process.
- Measles, Mumps, and Rubella vaccines can all be produced in non-fetal cell lines.[3]The Measles vaccine is produced in chicken eggs, human amnion cells from term placentas, and human kidney cultures from surgical samples. The Mumps vaccine is routinely produced using monkey cells, chick embryo fibroblasts, and embryonated chicken eggs. Rubella was the first vaccine that used animal cell lines (1969), but later work used fetalderived cell lines. Fetal cell lines are still in use today in the U.S. However, an ethical alternative is available in Japan.
- None of the 75 vaccines available in the US are produced using fresh fetal tissue.[4] A small number still use the historic cell “lines” derived from aborted fetal tissue harvested in the 60’s (WI-38 and MRC-5). Yet only three of these have no moral option in the US— all others are produced using ethical alternatives. This is because some manufactures, such as Merck, have not invested the time or money needed to produce ethical versions. This is not for scientific reasons, but likely because of the regulatory and costly burden that exists for such changes. For this reason, Rubella (and formulations that contain Rubella, such as MMR), chicken pox and Hepatitis A vaccines available in the US are still made with cells from aborted babies.
- Fetal tissue is not critical to the development of NEW vaccines to fight Zika and Ebola. Greater than 98% of research articles published on Zika do not use fetal tissue. Rather, adult blood cells recently led to a breakthrough in vaccine development for Cytomegalovirus (CMV), a virus affecting brain development in a way similar to Zika. Furthermore, a new successful Ebola vaccine was produced using monkey viro cells and the new shingles vaccine is grown in CHO cells (hamster).[5]
ETHICAL ALTERNATIVES
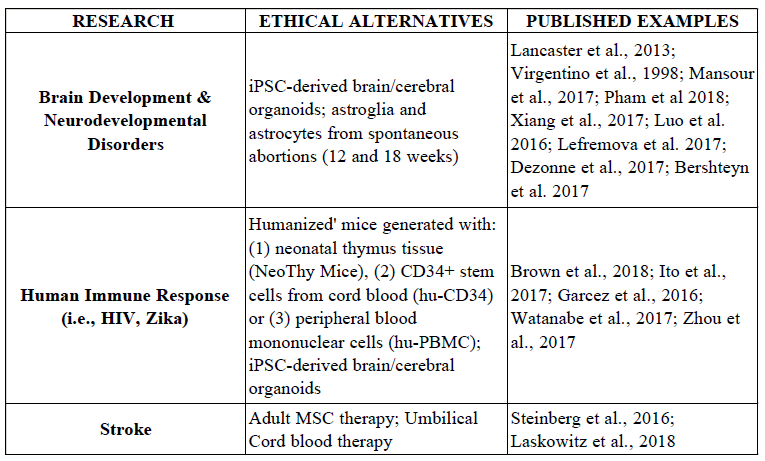
Ethical alternatives are available to researchers now. These include, but are not limited to, fresh human tissues from adult and pediatric populations, donated and discarded biopsies and surgical specimens, from both living and post-mortem individuals. There are numerous examples of investigators successfully using these ethical alternatives for research and clinical trials for studying the most complex processes, such as brain development and neurodevelopmental disorders[6], immune response to pathogens,[7] and stroke.[8]
Researchers have access to these ethical human tissue sources, which are available at several hospitals, academic institutions, and tissue banks across the nation, with proper consent and IRB approval. For example, tissue banks at the major academic institutions in my own state provide investigators with valuable discarded human tissue samples donated by patients, such as placenta, cord blood, and various tissues from surgeries and biopsies.[9] These tissues are valuable tissue resources for research and clinical practice.[10] For example, discarded cord blood from labor and delivery is stored in tissue repositories, because it is a rich and plentiful source of stem cells for research, regenerative medicine, and transplantation.[11] It is such a highly enriched source of adult stem cells, that it has become an important treatment option for a number of diseases, including blood disorders, diabetes, and traumatic brain injury. Up to 80 different diseases have been treated with cord blood thus far.[12] In addition, stem cells from placenta, amniotic fluid, and even a mother’s own bone marrow are even showing tremendous potential for in utero stem cell transplantation and treating the unborn BEFORE birth.[13] Perhaps one of the largest known tissue biorepositories is the National Marrow Donor Program (NMDP)- “Be The Match” for clinical transplants.[14] This registry includes more than 19 million individuals who stand ready to be a lifesaving bone marrow donor, as well as more than 249,000 cord blood units.[15] Adult stem cells from bone marrow and cord blood have saved the lives of over 1.5 million people worldwide.[16] My colleague, Dr. Prentice will be describing these studies in more detail.
iPS cells and organoids are an excellent source for studying development and disease. Scientists can “reprogram” adult somatic cells (such as skin cells) to make induced pluripotent stem cells (iPS cells) that possess an embryonic-like state.[17] Pluripotent stem cells (iPSCs, adult stem cells) can then be further reprogramed to generate “organoids”, also known as organs “in a dish”. Organoids are 3D cellular clusters replicating normal organ function in vitro for brain, liver, pancreas, intestine, stomach, lung, kidney, and eye.[18] These organoids have proven successful in modeling complex mechanisms, including Zika virus and microencephaly, hepatic development, neurodevelopmental (brain) disorders, retinal development, infectious disease, cancer and nephrogenesis (kidney). In a recent manuscript, the authors concluded, “the best advice at present is to rely on a combination of 2D and 3D organoid models…coupled with humanized animal models, to provide a comprehensive and reliable understanding of the molecular mechanisms involved in human diseases.”[19]
Post-mortem donations are a useful and ethical solution. Human cadavers are a valuable tissue source, from which stem cells can be isolated up to several days after death.[20] Spontaneous miscarriages and ectopic pregnancies are also an ethical alternative source of fetal tissue, and possibly stem cells, for research.[21] Low et al examined human fetal tissue from spontaneous abortions and predicted that over 100,000 miscarriages with Grade I/II quality tissue (viable cells and tissues from liver, thymus, spleen, bone marrow, pancreas, brain, spinal cord, kidneys, lungs, skin) could be available per year based on the estimated 750,000 miscarriages in the US annually.[22] However, such tissue (especially from miscarriages) is not easily accessible and commercially available like aborted fetal tissue. Future efforts could involve, (1) creating awareness and informing parents regarding the donation of their child’s remains to research as an anatomical gift and (2) redirected funds to establish fetal tissue banks to include a mechanism for obtaining tissue from miscarriages and ectopic pregnancies in a timely manner.
‘Humanized’ mice models can be generated using ethical sources. Fresh fetal tissue is currently collected from aborted fetuses to generate models called “humanized” mice to study infection and test therapeutics. Human fetal thymus and liver tissue, and sometimes fetal bones, are directly implanted into the mouse in an effort to generate a human immune system. These mice are used to study HIV/AIDS, evaluate potential HIV drugs, and investigate other infectious diseases, such as Ebola and cancer. A USCF research laboratory currently holds a $2-millionayear contract that uses human fetal tissue to generate ‘humanized’ mice models to test potential HIV drug targets. In addition, HHS is auditing department contracts that involve human fetal tissue and recently canceled a Food and Drug Administration contract that would obtain fetal tissue from ABR (referred for investigation to the Department of Justice by the House and Senate) to develop humanized mice. Some researchers argue that they ‘need’ human fetal tissue to generate the BLT (bone marrow, fetal liver, fetal thymus) humanized mouse model, because: (1) human fetal thymus tissue is best for selecting human T cells, and (2) hematopoietic (blood) stem cells from human fetal liver are needed for optional engraftment, and (3) implantation of human fetal bone fragments improves engraftment of the human cancer, multiple myeloma.[23] But in reality, similar stem cells can be obtained from ethical sources other than fetal liver, such as umbilical cord blood, bone marrow, and granulocyte colony-stimulating factor (G-CSF)-mobilized peripheral blood (MPB).[24] Furthermore, alternatives exist to the use of human fetal bones for generating humanized mouse models of multiple myeloma.[25]
The fact is, we do NOT need fresh fetal tissues for humanized mice, because ethical alternatives are available and being used now. A recent report showed that surplus human thymus tissue from newborn babies obtained during surgical procedures to repair congenital heart defects can be used to generate humanized mice. [26] The authors note that neonatal thymus tissue is “abundant” and “more than 1,000 fragments suitable for transplantation can be obtained from a single thymus”. In another example, two separate groups of researchers compared the efficacy of human cell engraftment using hematopoietic (blood) stem cells (HSCs) from cord blood, adult bone marrow, fetal liver, and MPB and found that human cord blood is the best scientific and ethical source for optimal human cell engraftment.[27] Stem cells from cord blood worked just as well as stem cells from fetal liver. The authors concluded that cord blood is comparable to fetal tissue and an appropriate source of stem cells. Therefore, surplus neonatal thymus tissue and cord blood obviates the need for other sources (i.e., fetal tissue, adult bone marrow), which have been argued as “required” in order to replicate the method routinely used to generate humanized mice.[28]
Other options for studying human immune response include the ability of researchers to purchase humanized mice from Jackson Laboratories for immediate shipment. Such models include the human CD34+ NSG humanized mouse (Hu-CD34 mice), developed using CD34+ stem cells from cord blood WITHOUT the use of human fetal tissues to provide the human growth factors necessary for engraftment. Hu-CD34 mice are “supreme in vivo models for long-term studies in the fields of immuno-oncology, infectious disease, and graft versus host disease”.[29] In addition, genetically-engineered NSG-SGM3 mice engrafted with CD34+ stem cells from cord blood are also available, which have increased CD33+ myeloid cell and CD4+ CD25+ FoxP3+ Treg cell numbers, which are key factors necessary for better engraftment of hematopoietic progenitor cells.[30] Finally, the NSG and NSG-SGM3 mice strains can also be engrafted with peripheral blood mononuclear cells (hu-PBMC mice) “for short-term experiments requiring mature T cells, including HIV infection, immuno-oncology, and graft-versus-host disease studies”.[31] Such ethical alternatives have been used to study HIV.[32]
In conclusion, it is clearly evident that numerous ethical alternatives exist and are available to researchers for studying some of the most complex diseases and disorders facing our nation today. I urge Congress and the Trump administration to stop using federal dollars to support aborted fetal tissue research and redirect funding to these ethical alternatives. If we continue to invest in fetal tissue research, this will delay future progress and advances using better and more ethical science.
Sincerely,
Tara Sander Lee, PhD
[1] https://www.hhs.gov/about/budget/fy2017/budget-in-brief/nih/index.html
[2] Salk JE, Recent Studies on Immunization against Poliomyelitis, Pediatrics 12, 471, 1953; and Salk JE et al., Formaldehyde Treatment and Safety Testing of Experimental Poliomyelitis Vaccines, Am. J. Public Health 44, 563, 1954; and Salk JE et al., Studies in Human Subjects on Active Immunization Against Poliomyelitis II. A Practical Means for Inducing and Maintaining Antibody Formation, Am. J. Public Health 44, 994, 1954; and Sabin AB, Present status of attenuated live-virus poliomyelitis vaccine, JAMA 162, 1589, 1956; https://lozierinstitute.org/history-of-fetal-tissue-research-and-transplants/#_ftn19
[3] https://cogforlife.org/wp-content/uploads/vaccineListOrigFormat.pdf; US House Select Investigative Panel Report, 2016
[4] https://cogforlife.org/wp-content/uploads/vaccineListOrigFormat.pdf; US House Select Investigative Panel Report, 2016
[5] US House Select Investigative Panel Report, 2016; Liu DX et al., Identification and expression of the human herpesvirus 6 glycoprotein H and interaction with an accessory 40K glycoproteinJ, Gen. Virol. 1993;74(9):1847-1857; Macagno A et al., Isolation of human monoclonal antibodies that potently neutralize human cytomegalovirus infection by targeting different epitopes on the gH/gL/UL128-131A complex, Journal of Virology. 2010;84(2):1005-1013
[6]Lancaster, MA et al., Cerebral organoids model human brain development and microcephaly, Nature. 2013, 501(7467); Virgintino D et al., Astroglia-microvessel relationship in the developing human telencephalon, Int. J. Dev. Biol., 1998, 42:1165-1168; Mansour AA et al., An in vivo model of functional and vascularized human brain organoids, Nat Biotechnol. 2018, 36(5):432-441; Pham MT et al., Generation of human vascularized brain organoids, Neuroreport, 2018, 2;29(7):588-593; Xiang Yet al., Fusion of Regionally Specified hPSC-Derived Organoids Models Human Brain Development and Interneuron Migration, Cell Stem Cell, 2017, 21(3):383-398; Luo C et al., Cerebral Organoids Recapitulate Epigenomic Signatures of the Human Fetal Brain, Cell Rep., 2016, 17(12):3369-3384; lefremova V et al., An Organoid-Based Model of Cortical Development Identifies Non-Cell-Autonomous Defects in Wnt Signaling Contributing to Miller-Dieker Syndrome, Cell Rep, 2017, 19(1):50-59; Dezonne RS et al., Derivation of Functional Human Astrocytes from Cerebral Organoids, Sci Rep, 2017, 7:45091; Bershteyn M et al., Human iPSC-Derived Cerebral Organoids Model Cellular Features of Lissencephaly and Reveal Prolonged Mitosis of Outer Radial Glia, Cell Stem Cell, 2017, 20(4):435-449
[7]Brown ME et al., A Humanized Mouse Model Generated Using Surplus Neonatal Tissue, Stem Cell Reports, 2018, 10(4):1175-1183; Ito R et al., Humanized mouse models: Application to human diseases, J Cell Physiol. 2018, 233:3723–3728; Garcez PP et al., Zika virus impairs growth in human neurospheres and brain organoids, Science 2016, 352:6287; Watanabe M et al., Self-Organized Cerebral Organoids with Human-Specific Features Predict Effective Drugs to Combat Zika Virus Infection, Cell Reports, 2017, 21, 517–532; Zhou T et al., High-Content Screening in hPSC-Neural Progenitors Identifies Drug Candidates that Inhibit Zika Virus Infection in Fetal-like Organoids and Adult Brain, Cell Stem Cell 2017, 21, 274–283
[8]Steinberg GK et al., Clinical Outcomes of Transplanted Modified Bone Marrow–Derived Mesenchymal Stem Cells in Stroke: A Phase 1/2a Study, Stroke, 2016 47(7): 1817–1824; Laskowitz DT et al., Allogeneic Umbilical Cord Blood Infusion for Adults with Ischemic Stroke: Clinical Outcomes from a Phase I Safety Study, Stem Cells Trans Med 2018;7:521–529
[9]Medical College of Wisconsin (http://pathology.mcw.edu/research/tissue-bank/); Blood Center of Wisconsin
(https://www.bcw.edu/bcw/Organ-Tissue-Marrow/index.htm); University of Wisconsin
(http://www.obgyn.wisc.edu/research/tissue-bank/reproductive-tissue-bank.aspx)
[10] Habibollah, S., Forraz, N., and McGuckin, C.P., Application of Umbilical Cord and Cord Blood as Alternative Modes for Liver Therapy in: N. Bhattacharya, P.G. Stubblefi eld (eds.), Regenerative Medicine: Using Non-Fetal Sources of Stem Cells (Springer-Verlag, London, 2015), 223-241.
[11] Roura S et al. The role and potential of umbilical cord blood in an era of new therapies: a review. Stem Cell Research & Therapy 2015 6:123; Baudin B et al. A protocol for isolation and culture of human umbilical vein endothelial cells. Nat. Protoc. 2007 2:481; Song RS et al. Generation, expansion, and differentiation of human induced pluripotent stem cells (hiPSCs) derived from the umbilical cords of newborns. Curr. Protoc. Cell Biol. 2014 29:1C16.1; http://www.nationalcordbloodprogram.org/
[12] http://www.nationalcordbloodprogram.org/qa/what_is_treated.html
[13] Couzin-Frankel, J. The Savior Cells? Science, 353:284, 2016; Fauza DO, Transamniotic stem cell therapy: a novel strategy for the prenatal management of congenital anomalies Pediatr Res, 2018, 83(1-2):241-248; Klein JD et al., Amniotic mesenchymal stem cells enhance normal fetal wound healing, Stem Cells Dev, 2011. 20(6):96976; Farmer D, Placental stem cells: The promise of curing diseases before birth. Placenta, 2017. 59:113-115; Di Bernardo J et al., Paracrine regulation of fetal lung morphogenesis using human placenta-derived mesenchymal stromal cells. J Surg Res, 2014. 190(1):255-63.
[14] https://bethematch.org/
[15] https://bethematch.org/about-us/how-we-help-patients/
[16] Gratwohl, A et al., One million haemopoietic stem-cell transplants: a retrospective observational study. Lancet Haematol, 2(3):91, 2015; Adult Stem Cell Research Facts: https://lozierinstitute.org/fact-sheet-adult-stemcellresearch-transplants/
[17] Choi J et al, A comparison of genetically matched cell lines reveals the equivalence of human iPSCs and ESCs, Nature Biotechnology 2015, 33:1173
[18] Habibollah S et al. Application of Umbilical Cord and Cord Blood as Alternative Modes for Liver Therapy in: N. Bhattacharya, P.G. Stubblefi eld (eds.), Regenerative Medicine: Using Non-Fetal Sources of Stem Cells (Springer-Verlag, London, 2015), 223-241, doi: 10.1007/978-1-4471-6542-2_22; Fatehullah A et al. Organoids as an in vitro model of human development and disease. Nature Cell Biology, 2016 18:3. For review: Lancaster M and Knoblich JA. Organogenesis in a dish: Modeling development and disease using organoid technologies, Science 2014, 345(6194):1247125
[19] Ho et al., Disease Modeling Using 3D Organoids Derived from Human Induced Pluripotent Stem Cells Int. J. Mol. Sci. 2018, 19:936
[20] S.I. Hodgetts, et al., Long live the stem cell: The use of stem cells isolated from post mortem tissues for translational strategies. The International Journal of Biochemistry & Cell Biology, 56:74–81, 2014.
[21] Moon et al., Preclinical Analysis of Fetal Human Mesencephalic Neural Progenitor Cell Lines: Characterization and Safety In Vitro and In Vivo, Stem Cell Trans Med 2016;5:1–13; Virgintino, D et al., Astoglia-microvessel relationship in the developing human telencephalon. Int. J. Dev. Biol. 1998, 42:1165; Kang X et al., Granulocytic myeloid-derived suppressor cells maintain feto-maternal tolerance by inducing Foxp3 in CD4+CD25-T cells by activation of the TGF-b/b-catenin pathway. Mol Hum Reprod, 2016, 22(7):499-511
[22] Low et al., Human fetal tissue from spontaneous abortions as potential sources of donor tissue for cell transplantation therapy. Transplantation Proceedings, 1994, 26 (6):3500
[23] Personal communication, Dr. Bryon Johnson
[24] Ito R et al., Humanized mouse models: Application to human diseases, J Cell Physiol. 2018, 233:3723–3728
[25] Lwin ST et al., Preclinical animal models of multiple myeloma, BoneKEy Reports 5, 2016, 772:1-9
[26] Brown ME et al., A Humanized Mouse Model Generated Using Surplus Neonatal Tissue, Stem Cell Reports, 2018, 10(4):1175-1183
[27] Lepus, CM et al., Comparison of human fetal liver, umbilical cord blood, and adult blood hematopoietic stem cell engraftment in NOD-scid/gammac-/-, Balb/c-Rag1-/-gammac-/-, and C.B-17-scid/bg immunodeficient mice. Human Immunology, 2009, 70(10), 790–802; Matsumura T et al., Functional CD5+ B cells develop predominantly in the spleen of NOD/SCID/gammac(null) (NOG) mice transplanted either with human umbilical cord blood, bone marrow, or mobilized peripheral blood CD34+ cells. Experimental Hematology, 2003, 31(9), 789–797. Also reviewed in Ito R et al., Humanized mouse models: Application to human diseases, J Cell Physiol. 2018, 233:3723–3728
[28] https://www.sciencemag.org/news/2018/12/report-nih-will-cancel-fetal-tissue-research-contract-fuelscontroversy; After reviewing the Brown et al. paper on NeoThy mice, Dr. Weissman argued that: “the technique it describes would require additional invasive procedures to withdraw bone marrow from the infant donors, in order to replicate the method used now to create humanized mice using fetal tissue.”
[29] https://www.jax.org/jax-mice-and-services/in-vivo-pharmacology/humanized-mice/cd34
[30] Billerbeck E et al., Development of human CD4+FoxP3+ regulatory T cells in human stem cell factor-,granulocyte-macrophage colony-stimulating factor-, and interleukin-3-expressing NOD-SCID IL2R{gamma}null
humanized mice. Blood, 2011, 117(11):3076-86. Jackson Labs website: https://www.jax.org/news-andinsights/jax-blog/2016/march/what-makes-nsg-sgm3-a-revolutionary-strain
[31]Jackson Labs website: https://www.jax.org/jax-mice-and-services/in-vivo-pharmacology/humanized-mice/pbmc
[32]Falkenhagen et al., Control of HIV Infection In Vivo Using Gene Therapy with a Secreted Entry Inhibitor, Molecular Therapy: Nucleic Acids, 2017, 9:132; Gorantla et al., CD8+ cell depletion accelerates HIV-1 immunopathology in humanized mice, J Immunol. 2010 184(12): 7082–7091; Heredia et al., Monotherapy with either dolutegravir or raltegravir fails to durably suppress HIV viraemia in humanized mice, J Antimicrob Chemother 2017; 72: 2570–2573