An Analysis of How Medicaid Expansion in Alaska Will Affect Abortion Rates

This is Issue 11 of the On Point Series.
Executive Summary
This month, the Alaska state legislature will consider legislation that would expand Alaska’s Medicaid program. This proposed Medicaid expansion will result in more women having easier access to taxpayer-funded abortion in Alaska – and may increase the number of abortions that occur. Medicaid expansion would place anywhere from 10,000 to 15,000 women of childbearing age onto a Medicaid program which both covers abortion and which currently pays for a very high percentage of the abortions performed in Alaska. Additionally, by guaranteeing Medicaid coverage to all low-income women – regardless of whether or not they are pregnant – the expansion would remove the incentive of many low-income women to carry their pregnancy to term. Finally, it would increase taxpayer funding for Planned Parenthood, the nation’s largest abortion provider and the locus of a significant number of abortions in Alaska. Overall, expanding Medicaid eligibility in Alaska will likely increase the overall incidence of abortion in the state.
Introduction
In the months leading up to the passage of the Affordable Care Act (commonly referred to as “ObamaCare”), a number of pro-life policy analysts expressed concern that the legislation could increase the incidence of abortion.[1] One major concern was that the Affordable Care Act would result in taxpayer subsidies of health insurance plans that cover abortion.[2] Others were concerned that the Affordable Care Act would indirectly subsidize abortion by generating additional revenue for Planned Parenthood. Finally, some feared that the Affordable Care Act would grant the U.S. Department of Health and Human Services the power to require that health insurance plans cover abortion-inducing drugs and devices.[3] However, the Affordable Care Act could also increase the incidence of abortion in another way; specifically, it allows states to expand Medicaid eligibility and, in many states, this amounts to increased access to abortion.
As originally written, the Affordable Care Act required each state to expand its Medicaid program to cover all adults under age 65 whose household incomes are less than or equal to 138 percent of the federal poverty level. States that failed to expand Medicaid would risk losing all federal funding for their Medicaid programs.[4] However, in June 2012, the United States Supreme Court ruled in National Federation of Independent Business v. Sebelius that the federal government could not require individual states to expand their Medicaid programs.[5] As such, states can decide for themselves if they want to expand Medicaid, without compromising their current federal Medicaid funding.
This month, the Alaska state legislature is considering a proposal by newly elected Governor Bill Walker to expand Medicaid eligibility as set forth in ObamaCare. There is a significant body of academic and policy research that shows that expanding eligibility for Medicaid dramatically increases Medicaid enrollment. Specifically, a recent analysis published by the Lewin Group indicates that Governor Walker’s proposal would increase Alaska’s Medicaid rolls anywhere from 40,000 to 55,000.[6] Much of the subsequent policy debate has centered around the cost to the taxpayers and how expanded Medicaid coverage would impact the quality of health care coverage for individuals already on Medicaid.
However, pro-lifers have expressed concerns that Medicaid expansion would result in more abortions in Alaska. In fact, there are several ways that Medicaid expansion would likely increase the incidence of abortion in Alaska. First, the expansion is projected to enroll anywhere from 10,000 to 15,000 women of childbearing age into a Medicaid program[7] which both covers abortion and which pays for a very high percentage of the abortions performed in Alaska. Second, by guaranteeing Medicaid coverage to all low-income women – regardless of whether they are pregnant – low-income women would lose the incentive to carry their pregnancy to term. Finally, Medicaid expansion would indirectly subsidize abortion by increasing the amount of taxpayer funding for Planned Parenthood, the nation’s largest abortion provider.
Background: Federal and State Policies Regarding Public Funding for Abortion
As legal access to abortion was expanded in the late 1960s and early 1970s, questions were raised about the extent to which state Medicaid programs should subsidize abortions for low-income women. Evidence from that time indicates that state Medicaid programs did provide reimbursement for eligible women obtaining abortions in states where it was legalized. After the Roe v. Wade decision legalized abortion in all 50 states,[8] a number of states took action to limit the extent to which their state Medicaid programs would pay for elective abortions.[9]
This resulted in a series of court cases culminating in the Beal v. Doe,[10] Maher v. Roe,[11] and Poelker v. Doe[12] decisions in 1977 in which the Supreme Court held that the government is not required to fund elective abortions either under federal statute or the U.S. Constitution. Meanwhile, in 1976 Congress passed an appropriations limitation known as the Hyde Amendment which restricted federal Medicaid funds for abortions. This resulted in another round of litigation. In 1980, the Supreme Court ruled in Harris v. McRae[13] that the federal Hyde Amendment was constitutional.[14]
Since that time, the federal funding of abortions has been largely limited to situations where either the abortion was performed to save the life of the woman or when the pregnancy resulted from rape or incest.[15] However, states have always been free to use their own tax dollars to fund abortions through their respective state Medicaid programs. Currently 17 states, including Alaska, fund abortions through their state Medicaid programs.[16]
The History of Taxpayer-Funded Abortion in Alaska
Alaska was one of only a few states to legalize abortion prior to the Supreme Court’s 1973 Roe v. Wade decision. Specifically, on July 29, 1970[17] an Alaska statute took effect, legalizing abortion before the viability of the unborn child. Surveys performed throughout the 1970s and 1980s show that at least since June 1973, Alaska has paid for abortions under its Medicaid program without special limitations. Currently, state Medicaid funds are available for all medically necessary abortions.[18]
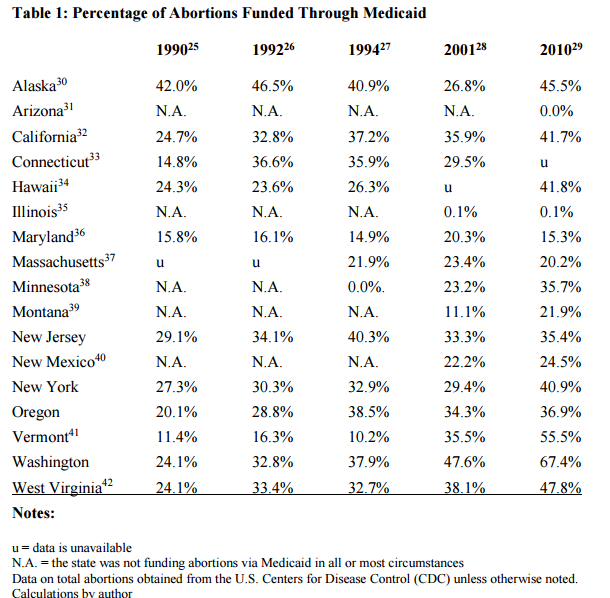
However, simply because a state has a policy of funding abortions for women on Medicaid does not mean a significant number of abortions are actually funded in practice. Indeed, there exists significant variance in the funding practices among the 17 states that publicly fund abortion through Medicaid. For instance, a 1994 opinion by the Circuit Court of Cook County required Illinois to provide reimbursement “for abortions necessary to protect a woman’s health.”[19] However, a very low percentage of abortions performed in Illinois are publicly funded through Medicaid (Table 1). Similarly, in 1995 a Federal District court required Montana to publicly fund “medically necessary” abortions through Medicaid.[20] However, a relatively small percentage of the abortions taking place in Montana are actually paid for by Medicaid (Table 1).
The Guttmacher Institute has released state-level data on taxpayer-funded abortions for a select group of years. According to their data, it is relatively rare for a state to fund more than 40 percent of its abortions through Medicaid (Table 1).[21] However, the percentage of abortions that are publicly funded in Alaska is frequently over 40 percent. This is one of the highest rates in the country.
This disparity has come to the attention of both pro-life activists and legislators in Alaska. In April 2014, SB 49 was signed into law by then-Governor Sean Parnell. SB 49 would have limited Medicaid funding of abortion to circumstances where the abortion was the result of rape or incest or where the abortion was “medically necessary.” Furthermore, it defined “medically necessary” as a situation where a physician felt that an abortion must be performed to avoid “serious risk to the life or physical health of a woman.”[22] SB 49 also required doctors to select from a list of 21 pre-approved reasons why an abortion would be “medically necessary.”[23] However, SB 49 was subsequently enjoined by an Alaska State Court and is currently not in effect.[24]
The Impact of Medicaid Funding on the Incidence of Abortion
So what impact does public funding of abortion through Medicaid have on the incidence of abortion? A 2009 Guttmacher Institute literature review identified 18 peer-reviewed studies that analyzed the impact of state Medicaid funding on the incidence of abortion.[43] These methodologically diverse studies utilized abortion data from a variety of sources. Overall, of the 18 studies they considered, 15 found statistically significant evidence that abortion rates went up after Medicaid funding was increased.[44] Two additional studies not included in the Guttmacher analysis also provide strong evidence that Medicaid funding of abortion increases the incidence of abortion.[45]
These findings held for studies using time series cross-sectional data to analyze overall abortion rates.[46] They also held for studies using time series cross-sectional data to specifically analyze teen abortion rates.[47] They held as well for studies that analyzed abortion rates in smaller groups of states[48] and for two studies that specifically analyzed the impact of public funding restrictions on pregnancy outcomes in North Carolina.[49]
The studies that analyzed data from North Carolina were especially interesting. From 1980 to 1995 North Carolina taxpayers funded abortion for low-income women – not through Medicaid, but through a state abortion fund that periodically ran out of money. Whenever funds were depleted, the researchers found there were statistically significant decreases in the abortion rate and, months later, statistically significant increases in the birth rate.[50] These findings were statistically stronger when the pregnancy outcomes for African American women were considered. Overall, the authors concluded that 37 percent of the women who would have otherwise had an abortion carried their child to term when funding was not available.[51]
The authors of the Guttmacher literature review acknowledge that the best research indicates that Medicaid funding increases the incidence of abortion: they state that “the best studies…used detailed data from individual states and compared the ratio of abortions to births both before and after the Medicaid restrictions took effect.[52] These found that 18-37 percent of pregnancies that would have ended in Medicaid funded abortions were carried to term when funding was no longer available.”[53] Looking at this another way, according to Guttmacher, the methodologically strongest studies found that Medicaid funding of abortion increases the abortion rate for women on Medicaid by anywhere from 22 percent to 58 percent.[54]
Impact of Medicaid Expansion on the Incidence of Abortion in Alaska
When the Affordable Care Act was signed into law, it required each state to expand its Medicaid program to cover all adults under age 65 whose household incomes are less than or equal to 138 percent of the federal poverty level.[55] However, in June 2012, the United States Supreme Court ruled in National Federation of Independent Business v. Sebelius that the federal government could not require individual states to expand their Medicaid programs for adults.[56] As a result, states now have the option to reject the Medicaid expansion provision of the Act without compromising their current federal Medicaid funding.
Since that time, approximately 30 states have expanded their Medicaid program in this manner. Alaska is not among them. Former Alaska Governor Sean Parnell consistently opposed Medicaid expansion, calling it a “failed experiment.”[57] However, Alaska’s new Governor Bill Walker has made Medicaid expansion a high priority. He argues that because roughly 40,000 Alaskans would receive health care coverage through Medicaid and the federal government would pay a high percentage of the costs, Medicaid expansion is the best way forward for the state.[58] But Walker overlooks the various moral quandaries that expansion proposes – not the least of which is the fact that the expansion of Medicaid is likely to result in a higher incidence of taxpayer-funded abortion in the state. Overall, this Medicaid expansion will likely increase the incidence of abortion in Alaska in at least four ways.
1) Medicaid Expansion Would Directly Place 10,000 to 15,000 Additional Women onto a Medicaid Health Insurance Plan That Covers Abortion
There is an impressive body of policy and academic research that shows that increasing eligibility for Medicaid increases state Medicaid rolls.[59] In particular, a 2013 analysis published by the Lewin Group indicates that increasing Medicaid eligibility to 138 percent of the poverty line would increase Alaska’s Medicaid rolls by anywhere from 40,000 to 55,000 people.[60] This analysis also indicates that Medicaid expansion would result in anywhere from 10,000 to 15,000 additional women of childbearing age (21-44) receiving health care coverage through Medicaid.[61] As was mentioned earlier, in Alaska pregnant women whose income does not exceed 175 percent of the federal poverty line are eligible for Medicaid – and get their abortion publicly funded.[62] That said, a pregnant woman seeking a publicly funded abortion has to apply to enroll in Medicaid and then face a wait of up to 30 days for the application to be processed.[63] It is possible that the application process and the delay may dissuade some Alaskan women from seeking abortions. However, if Medicaid is expanded, many of those women of childbearing age will already be enrolled in Medicaid. They will not have to apply to enroll in Medicaid and they will not face a delay. Overall Medicaid expansion will give thousands of Alaskan women faster and easier access to taxpayer-funded abortions.
Additionally, in every state, a certain percentage of individuals who are already eligible for Medicaid are not enrolled in the program. But under Medicaid expansion, a high percentage of these individuals are expected to enroll, due to increased publicity and awareness of Medicaid that comes with expansion. This effect is often referred to as the “woodwork effect.” Not only will states have to pay the traditional match rate for these already-eligible enrollees, but this will increase the number of individuals who are enrolled in Medicaid, giving them faster and easier access to taxpayer-funded abortion. Without expansion, they may never enroll. With expansion, they will enroll and, as a result, they will have easier access to abortion.
2) Medicaid Expansion Would Result in Women Leaving Non-Abortion-Providing Insurance Plans to Enroll in Abortion-Covering Medicaid
In Alaska and other states that have not expanded Medicaid, individuals whose income exceeds 100 percent of the poverty line are currently eligible to purchase subsidized insurance plans through a federally-facilitated health care exchange.[64] However, if Medicaid were expanded to 138 percent of the poverty line, some individuals who are currently in exchange plans would become eligible for Medicaid. A recent analysis by the Urban Institute indicates that if Medicaid expands in Alaska, 3,000 women of childbearing age who are currently eligible for exchange plans would then become eligible for Medicaid.[65] Furthermore, a significant percentage of these people would likely enroll in Medicaid since it would be significantly less costly.
This phenomenon has played out in other states that have expanded Medicaid eligibility. In the mid-1990s, Delaware began to expand its Medicaid eligibility to include childless adults earning up to 100 percent of the federal poverty level. Between 2002 and 2011 the rate of private insurance in Delaware dropped by 10 percentage points, while Medicaid enrollment increased by 7 percentage points. Arizona and Maine have seen similar results after they expanded eligibility for their state Medicaid programs.[66]
Furthermore, a Lozier Institute analysis found that many of the insurance plans on Alaska’s federally-facilitated health insurance exchange do not cover abortion. Currently, Alaska has only two providers[67] on its health insurance exchange[68]– Moda Health, which offers 10 insurance plans, and Premera Blue Cross Blue Shield of Alaska, which offers 18 multi-state plans. Of these 28 combined plans, 12 cover abortion and 16 do not.[69] As such, the Medicaid expansion would likely result in a significant number of women choosing to leave exchange- based plans that do not cover abortion in favor of a state Medicaid program that does cover abortion.
3) Medicaid Expansion Would Remove the Incentive for Low-Income Alaskan Women to Carry Their Pregnancies to Term
In Alaska, if a pregnant woman with no children (who is below 175 percent of Federal Poverty Level) obtains an abortion, she also loses her eligibility for Medicaid. Medicaid has traditionally not covered able-bodied, non-pregnant, and childless adults. And so after a childless woman is no longer pregnant in Alaska, she is no longer eligible to receive Medicaid benefits. As such, the Medicaid coverage that is limited to pregnant women and mothers creates an incentive for some women to carry their pregnancy to term. However, if Medicaid is expanded, a childless woman at or below 138 percent of the Federal Poverty Line will retain Medicaid coverage whether she carries her pregnancy to term or not. As such, the incentive for women to carry their pregnancy to term vanishes and, as a result, the incidence of abortion is likely to increase.
4) Medicaid Expansion Would Result in More Taxpayer Funding for Planned Parenthood
Planned Parenthood operates four centers in Alaska; one in Anchorage, one in Fairbanks, one in Juneau, and one in Soldotna.[70] According to their website, three of those four facilities perform abortions.[71] A 2011 Guttmacher report indicates that there are nine abortion providers in Alaska and four abortion clinics.[72] As such, a significant percentage of the abortion facilities in Alaska are Planned Parenthood affiliates. Furthermore, Alaska Dispatch News has referred to Planned Parenthood as the biggest abortion provider in Alaska.[73]
Planned Parenthood publicly advocates for Medicaid expansion.[74] On its website, Planned Parenthood states that 36 percent of women receiving publicly funded family planning receive their care at Planned Parenthood centers.[75] As such, an expansion of Medicaid would increase the amount of funding Planned Parenthood would receive for contraception and a range of other services. While this money would not be directly funding abortion, it would still be indirectly subsidizing abortion by funding a healthcare provider that performs a significant number of abortions in Alaska. A number of states, including Arizona, Kansas, North Carolina, Tennessee, and Texas, have passed legislation preventing funding from the state’s Medicaid program from going to providers that also perform abortions.[76] However, no such legislation has been enacted in Alaska.
Conclusion
Pro-lifers have good reason to oppose Governor Walker’s proposal to expand Medicaid coverage in Alaska. It would place between 10,000 and 15,000 women of childbearing age directly onto a Medicaid program that covers abortion and which already pays for a disproportionately high percentage of abortions that are performed in Alaska. Additionally, by guaranteeing Medicaid coverage to all low-income women – and not just pregnant, low-income women – it removes an important incentive for many women to carry their pregnancy to term. It would also indirectly subsidize abortion by providing more taxpayer funding for Planned Parenthood. There is a broad body of academic research that shows that subsidizing abortions through Medicaid increases state abortion rates. Pro-lifers would do well to oppose Governor Walker’s Medicaid expansion proposal.
Michael J. New, Ph.D. is an Associate Scholar for the Charlotte Lozier Institute and Assistant Professor at University of Michigan-Dearborn.
*The author would like to thank Lozier Institute Research Assistant Genevieve Plaster for her assistance with some of the research and data collection.
[1] Susan B. Anthony List. “Taxpayer Abortion Funding in Obamacare.” http://www.sba-list.org/taxpayer-funding-aca (May 10, 2015).
[2] Susan B. Anthony List.
[3] Susan B. Anthony List.
[4] Cole M et al., An Analysis of Medicaid Expansion in Alaska. Falls Church, VA: The Lewin Group, 2013.
http://dhss.alaska.gov/Documents/Lewin_Final_Report.pdf (Page 4) (May 10, 2015).
[5] Cole M et al., 2013.
[6] Cole M et al., 2013.
[7] Cole M et al., 2013.
[8] Roe v. Wade, 410 U.S. 113 (1973).
[9] Merz JF, Jackson CA, Klerman JA. A Review of Abortion Policy: Legality, Medicaid Funding, and Parental Involvement, 1967-1994. Women’s Rights Law Reporter. 1995;17(1):1-62.
[10] Beal v. Doe, 432 U.S. 438 (1977).
[11] Maher v. Roe, 432 U.S. 464 (1977).
[12] Poelker v. Doe, 432 U.S. 519 (1977).
[13] Harris v. McRae, 448 U.S. 297 (1980).
[14] Merz, Jackson, and Klerman, 1995.
[15] Merz, Jackson, and Klerman, 1995.
[16] Guttmacher Institute. State Policies in Brief. “State Funding of Abortion Under Medicaid.” New York: Guttmacher Institute, 2015. http://www.guttmacher.org/statecenter/spibs/spib_SFAM.pdf (May 11, 2015).
[17] Merz, Jackson, and Klerman, 1995.
[18] Merz, Jackson, and Klerman, 1995.
[19] Merz, Jackson, and Klerman, 1995.
[20] Merz, Jackson, and Klerman, 1995.
[21] For the 66 state-years for which data is available, the percentage of abortions funded by Medicaid has exceeded 40 percent only 11 times (Table 1).
[22] Public Health Watch. Alaska Republicans Pass Law Allowing Alaska Republicans to Tell Doctors What Qualifies As A ‘Medically Necessary’ Abortion. April 19, 2014. https://publichealthwatch.wordpress.com/2014/04/19/alaska-republicans-pass-law-allowing-alaska-republicans-tell-doctors-what-qualifies-as-a-medically-necessary-abortion/ (May 10, 2015).
[23] Public Health Watch, 2014.
[24] Blumberg P. Alaska Abortion Limits for Medicaid Patients Put on Hold. Bloomberg Business, February 5, 2015. http://www.bloomberg.com/news/articles/2014-02-05/alaska-abortion-limits-for-medicaid-patients-put-on-hold; (May 11, 2015); Center for Reproductive Rights. Planned Parenthood of the Great Northwest v. Steur, September 15, 2014. http://www.reproductiverights.org/case/planned-parenthood-of-the-great-northwest-v-streur (May 11, 2015).
[25] Data on publicly funded abortions in 1990 obtained from Gold RB, Daley D. Public Funding for Contraceptive, Sterilization and Abortion Services, Fiscal Year 1990. Family Planning Perspectives. 1991; 23: 204-211.
[26] Data on publicly funded abortions in 1992 obtained from Gold RB, Daley D. Public Funding for Contraceptive, Sterilization and Abortion Services, Fiscal Year 1992. Family Planning Perspectives. 1993, 25: 244-251.
[27] Data on publicly funded abortions in 1994 obtained from Sollom T, Gold RB, Saul R. Public Funding for Contraceptive, Sterilization and Abortion Services, 1994. Family Planning Perspectives. 1996; 28: 166-173.
[28] Data on Publicly Funded abortions in 2001 obtained from Sonfield A and Gold RB, Public Funding for Family Planning, Sterilization and Abortion Services, FY 1980–2001, New York: Guttmacher Institute, 2005.
[29] Data on publicly funded abortions in 2010 obtained from Sonfield A and Gold RB, Public Funding for Family Planning, Sterilization and Abortion Services, FY 1980–2010, New York: Guttmacher Institute, 2012.
[30] Alaska did not release state abortion data to the CDC in 2001. I estimated 2,000 abortions were performed on Alaska residents in 2001 using data from the Guttmacher Institute.
[31] The Arizona Supreme Court’s ruling requiring Arizona to publicly fund medically necessary abortions for low-income women was not issued until 2002.
[32] California did not release state abortion data to the CDC in 2001, 2006, or 2010. Their abortion totals are estimated using figures from the Guttmacher Institute.
[33] In 1990 and 1994, Connecticut released the amount of money spent on publicly funded abortions, but not the number of publicly funded abortions performed. Based on the ratio of funding to abortions performed in other states, I estimate that Connecticut publicly funded 2,775 abortions in 1990 and 5,302 abortions in 1994. Connecticut did not release data on the number of publicly funded abortions in 2010.
[34] Hawaii did not release a complete data on the number of publicly funded abortions in either 2001 or 2006.
[35] The Circuit Court of Cook County’s ruling requiring Illinois to publicly fund medically necessary abortions for low-income women was not issued until December 1994.
[36] Maryland did not release state abortion data to the CDC in 2010. Their abortion totals are estimated using figures from the Guttmacher Institute.
[37] Massachusetts did not release any data on publicly funded abortions in either 1990 or 1992. In 1994, Massachusetts released the amount of money spent on publicly funded abortions, but not the number of publicly funded abortions performed. Based on the ratio of funding to abortions performed in other states, I estimate that Massachusetts publicly funded 7,037 abortions in 1994.
[38] The state court ruling requiring Minnesota to fund all medically necessary abortions for low-income women was not issued until June 16, 1994. Guttmacher indicates that no abortions were publicly funded in Minnesota in 1994.
[39] In 2001 and 2006, Montana released the amount of money spent on publicly funded abortions, but not the number of publicly funded abortions performed. Based on the ratio of funding to abortions performed in other states, I estimate that Montana publicly funded 232 abortions in 2001 and 127 abortions in 2006.
[40] New Mexico’s Human Services Department did not expand Medicaid coverage to include medically necessary abortions until December 1, 1994.
[41] Vermont did not release data on publicly funded abortions in 2006.
[42] In 2006 West Virginia released the amount that was spent on publicly funded abortions, but not the number performed. Based on the ratio of funding to abortions performed in other states, I estimate that West Virginia publicly funded 546 abortions in 2006.
[43] Henshaw SK et al., Restrictions on Medicaid Funding for Abortions: A Literature Review. New York: Guttmacher Institute, 2009.
[44] Calculation by author.
[45] New MJ. Analyzing the Effect of Anti-Abortion U.S. State Legislation in the Post-Casey Era. State Politics and Policy Quarterly. 2011;11(1) 28-47; New MJ. Analyzing the Effect of U.S. Anti-Abortion Legislation in the Post-Casey Era: A Reassessment. State Politics and Policy Quarterly. 2014; 14(3): 228-268.
[46] Hansen, SD. State Implementation of Supreme Court Decisions: Abortion Rates Since Roe v. Wade. Journal of Politics. 1980; 42(2): 372-395; Haas-Wilson D. The Economic Impact of State Policy Restrictions on Abortion: Parental Consent and Notification Laws and Medicaid Funding Restrictions. Journal of Policy Analysis and Management. 1993; 12: 498-511; Haas-Wilson D. Women’s Reproductive Choices: The Impact of Medicaid Funding Restrictions. Family Planning Perspectives. 1997; 29(5): 228-233; Meier KJ, McFarlane D. State Family Planning and Abortion Expenditures: Their Effect on Public Health. The American Journal of Public Health. 1994; 84(9): 1468-1472; Blank R, George C, London R. “State Abortion Rates: The Impact of Policies, Providers, Politics, Demographic, and Economic Environment. Journal of Health Economics. 1996; 15(5): 513-553; Meier KJ, Haider-Markel D, Stanislawski A, MacFarlane D. The Impact of State Level Restrictions on Abortion. Demography. 1996; 33: 307-312; Levine P, Trainor A, Zimmerman D. “The Effect of Medicaid Abortion Restrictions on Abortions, Pregnancies, and Births. Journal of Health Economics. 1996; 15(5): 555-578; Matthews S, Ribar D, Wilhelm M. The Effects of Economic Conditions and Access to Reproductive Health Services on State Abortion Rates and Birthrates. Family Planning Perspectives. 1997; 29(2): 52-60.
[47] Lundberg S, Plotnick RD. Effects of State Welfare Abortion and Family Planning Policies on Premarital Childbearing on White Adolescents. Family Planning Perspectives. 1990; 22(6): 246-275; Haas-Wilson D. The Impact of State Abortion Restrictions on Minors’ Demand for Abortions. Journal of Human Resources. 1996; 31:140-158.
[48] Trusssel J, Menken J, Lindheim B, Vaughn, B. The Impact of Restricting Medicaid Funding for Abortion. Family Planning Perspectives. 1980; 12(3):120-123 & 127-130; Korenbrot C, Brindis D, Priddy, F. Trends in Rates of Live Births and Abortions Following State Restrictions on Public Funding of Abortion. Public Health Reports. 1990; 105(6):555-562.
[49] Cook PJ et al., The Effects of Short Term Variation in Abortion Funding on Pregnancy Outcomes. Journal of Health Economics. 1999; 18(2): 241-257; Morgan PS, Parnell, AM. Effect of Pregnancy Outcomes of Charges in the North Carolina State Abortion Fund. Population Research and Policy Review 2002; 21:319-338.
[50] Cook PJ et al., 1999; Morgan PS, Parnell, AM, 2002.
[51] Cook PJ et al., 1999; Morgan PS, Parnell, AM, 2002.
[52] Henshaw SK et al., 2009.
[53] Henshaw SK et al., 2009.
[54] Calculation by author.
[55] Cole M et al., 2013.
[56] Cole M et al., 2013.
[57] Andrews L. New Report Says Medicaid Expansion Will Save Alaska Money. Alaska Dispatch News, February 6, 2015. http://www.adn.com/article/20150206/new-report-says-medicaid-expansion-will-save-alaska-money (May 10, 2015).
[58] Feidt A. Alaska’s Governor Eager to Expand Medicaid. National Public Radio, December 16, 2014. http://www.npr.org/blogs/health/2014/12/16/370979687/alaskas-governor-eager-to-expand-medicaid (May 10, 2015).
[59] Piper JM, Mitchel EF, Ray WA. Expanded Medicaid Coverage for Women to 100 Percent of the Federal Poverty Level. American Journal of Preventive Medicine. 1994; 10(2): 97-102; Dubay L, Kenney G. The Effects of Medicaid Expansion on Insurance Coverage for Children. The Future of Children. 1996; 6(1): 152-161; Sommers BD, Baicker K, Epstein AM. Mortality and Access to Care Among Adults After State Medicaid Expansions. The New England Journal of Medicine. 2012; 367: 1025-1034.
[60] Cole M et al., 2013.
[61] Cole M et al., 2013.
[62] National Network of Abortion Funds. Can Medicaid Cover My Abortion? 2014. http://www.fundabortionnow.org/get-help/medicaid#AK (May 10, 2015).
[63] National Network of Abortion Funds, 2014.
[64] Healthcare.gov. Incomes that Qualify for Lower Costs: Alaska/Hawaii https://www.healthcare.gov/qualifying-for-lower-costs-ak-hi/; (May 11, 2015). 2014 Poverty Rate Data obtained from U.S. Department of Health and Human Services. 2014 Poverty Guidelines. http://aspe.hhs.gov/poverty/14poverty.cfm (May 11, 2015).
[65] Kenney G et al., Opting in to the Medicaid Expansion Under the ACA: Who Are the Uninsured Adults Who Could Gain Health Care Coverage? Washington, DC: Urban Institute 2012. http://www.urban.org/research/publication/opting-medicaid-expansion-under-aca/view/full_report (Calculation by author using figures from Appendix Table 3 and Appendix Table 8.)
[66] Ingram J. Medicaid Expansion We Already Know How the Story Ends. Foundation for Government Accountability. March 11, 2013. http://uncoverobamacare.com/wp-content/uploads/2013/10/Medicaid-Expansion-UncoverObamaCare.pdf (May 12, 2015).
[67] State of Alaska. Department of Commerce, Community, and Economic Development. “ACA Special Enrollment Period Announced.” 2015. http://commerce.state.ak.us/pub/PR-15-005-ACA-SpecialEnrollmentPeriodAnnounced.pdf (May 11, 2015).
[68] State of Alaska. Department of Commerce, Community, and Economic Development. Division of Insurance. “Affordable Care Act: What It Means For You.” http://commerce.state.ak.us/dnn/ins/AffordableCareAct/Exchanges.aspx (May 11, 2015).
[69] Family Research Council and Charlotte Lozier Institute. “Abortion in Obamacare: Alaska.” http://www.obamacareabortion.com/alaska (May 11, 2015).
[70] Planned Parenthood. Health Center Search Results: Alaska. http://www.plannedparenthood.org/health-center/AK (May 10, 2015).
[71] Planned Parenthood. Health Center Search Results: Alaska. http://www.plannedparenthood.org/health-center/AK (May 11, 2015). Calculation by author.
[72] Guttmacher Institute. State Facts About Abortion: Alaska. 2014. https://www.guttmacher.org/pubs/sfaa/pdf/alaska.pdf (May 11, 2015).
[73] Demer L. Voters Approve Measure Requiring Abortion Notification. Alaska Dispatch News, August 25, 2010. http://www.adn.com/article/20100825/voters-approve-measure-requiring-abortion-notification (May 11, 2015).
[74] Planned Parenthood. “How Will Medicaid Expansion Help Women.” http://www.plannedparenthoodaction.org/issues/medicaid-and-women/medicaid-expansion-and-women/ (May 11, 2015).
[75] Planned Parenthood. “Medicaid Expansion 101.” 2013. http://www.plannedparenthoodaction.org/files/2913/6269/3475/Medicaid_Expansion_030613_vF.pdf (May 11, 2015).
[76] Baker S. Efforts to Cut Funding For Planned Parenthood at State Level Fall Short. The Hill, October 27, 2012. http://thehill.com/policy/healthcare/264439-efforts-to-cut-state-funding-for-planned-parenthood-fall-short (May 12, 2015).