











Montana’s vital statistics report for 2018 was published by the Montana Department of Public Health and Human Services in December 2019. The report shows that abortions reported in Montana increased from 2017.
Changes in Montana Abortions, 2017-2018

The report does not include information on Planned Parenthood’s Montana market share.
Abortion Totals and Trends
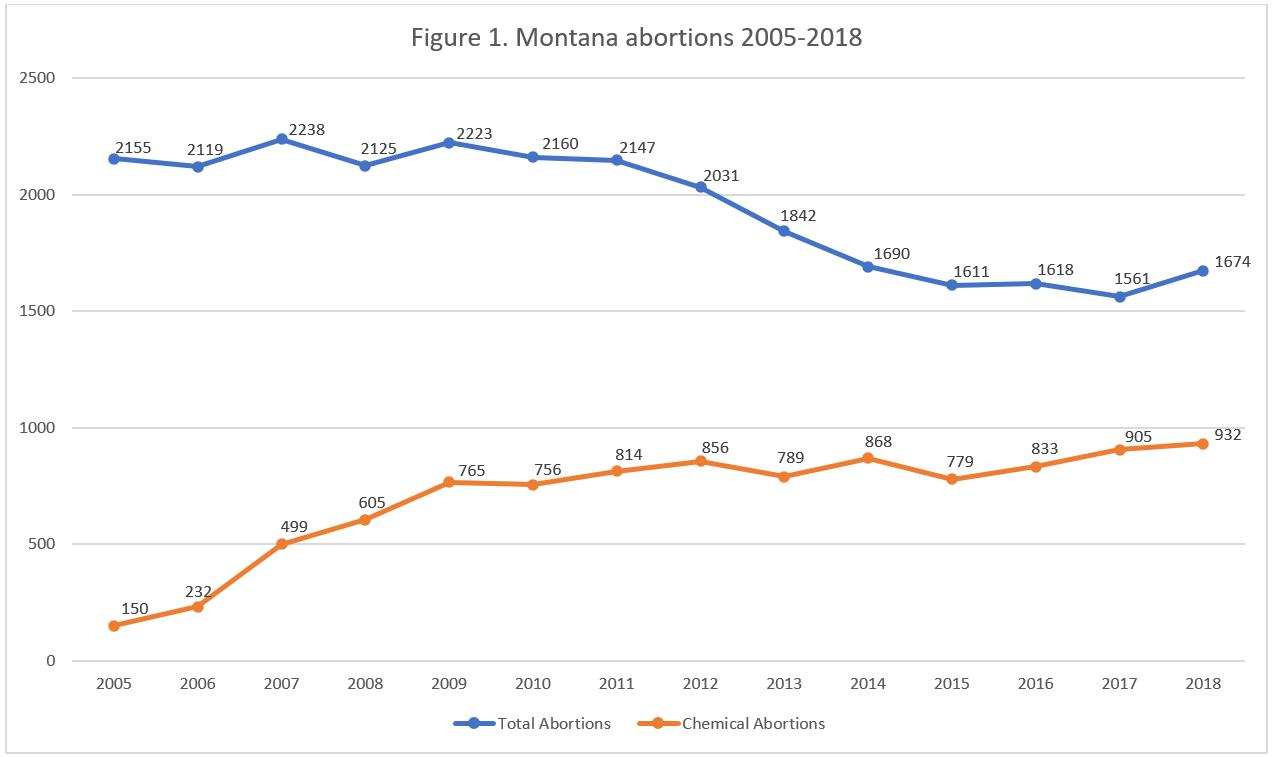
In 2018, there were 1,674 abortions reported in Montana (Fig. 1). This was an increase of seven percent from the previous year. Chemical abortions increased by three percent over the same time period, making up 56 percent of all Montana abortions in 2018. The Charlotte Lozier Institute estimates that Montana’s abortion rate in 2018 was 8.7 abortions per 1,000 women of childbearing age, an increase from 2017 but still well below the national rate (Fig. 2).
State Report Summary
A majority of the abortions reported in Montana in 2018, that is, 90 percent, were performed on Montana residents. Fifty-seven percent of Montana abortions were on women in their twenties, including 29 percent on women ages 20 to 24 and 28 percent on women ages 25 to 29. Twenty-nine percent were on women in their thirties. Eleven percent of the abortions were performed on girls ages 15 to 19 and four percent on women age 40 or older. Montana suppresses numbers smaller than five in order to protect women’s privacy, and the precise number of girls under the age of 15 who got abortions in Montana was suppressed.
Eighty-eight percent of the abortions occurring in Montana were on white women. Eight percent were on American Indian or Alaska Native women, and three percent were on women of other races. This is similar to the racial makeup of Montana’s population of women of childbearing age; in 2018, 89 percent of Montana women between the ages of 15 and 44 were white, eight percent were American Indian or Alaska Native, two percent were Asian, and one percent were African American.
Forty-seven percent of the abortions performed in Montana were on women with no previous live births. Twenty percent had one previous live birth, and 32 percent had more than one. Most of the abortions were performed on women who had had an abortion before; 41 percent had one previous abortion and 21 percent had two or more, compared to 38 percent with no previous abortions.
Well over half the abortions reported in Montana (56 percent) were chemical abortions, while 44 percent were surgical abortions. There were no intrauterine instillation abortions or hysterectomy or hysterotomy abortions reported in 2018. Two-thirds of the abortions were performed at eight weeks of gestation or earlier. Twenty-four percent were performed between nine and 13 weeks and three percent between 14 and 15 weeks of gestation. Two percent each were performed between 16 and 17 and 18 and 20 weeks. There were 10 abortions, 0.6 percent of the total, reported at 21 weeks of gestation or later.
Montana Joins the TelAbortion Study
Chemical abortions are likely to show an increase in Montana’s next report. Starting in November of 2019, Planned Parenthood of Montana began participating in the TelAbortion Study, a project that is experimenting with a new model of chemical abortion. Normally, a woman who seeks a chemical abortion visits an abortion center, receives an examination, and is given the abortion pills by an abortion provider who has been licensed to distribute them. The first pill in the chemical abortion regimen, mifepristone, is a dangerous drug and is subject to a Risk Evaluation and Mitigation Strategy (REMS) that requires distributers to be capable of caring for women who experience complications. The REMS prohibits mifepristone from being dispensed at pharmacies. However, in the TelAbortion Study, women do not meet with their abortion providers face-to-face. Instead, women get a checkup at a local health care facility, video conference with the abortion provider, and have the abortion pills mailed to them.
In September 2019, the results of the TelAbortion study thus far were published, revealing that nine of the women who had taken mifepristone as part of the study required a procedure to complete their abortions. Also, 16 women went to an emergency room or urgent care department – 14 for bleeding and pain, one for dizziness, and one to receive Rh immune globulin. At least two women were hospitalized – one for experiencing a seizure during an aspiration abortion performed due to bleeding, the other for severe anemia. In all, 248 women were sent packages of abortion pills as part of the study. However, abortion outcomes were unknown for nearly a quarter of the women, and two women decided not to take the mifepristone and continued their pregnancies.
State Ranking
In 2016, Montana’s abortion reporting quality was ranked at 23rd place by a Charlotte Lozier Institute survey of abortion reporting across the country. Montana has made improvements over the past three years. However, the Treasure State could continue to make progress by including information that it already collects on women’s marital status and level of education. Montana’s abortion reporting form collects information on babies who are born alive during abortions, but the Montana Department of Public Health and Human Services cautioned CLI that this data can be unreliable, and it has not retained the data in its abortion data system. Montana could consider strengthening its protections for abortion survivors, including better data collection. Montana could also report information on the facilities where abortions occur and the methods of payment used to fund abortion.
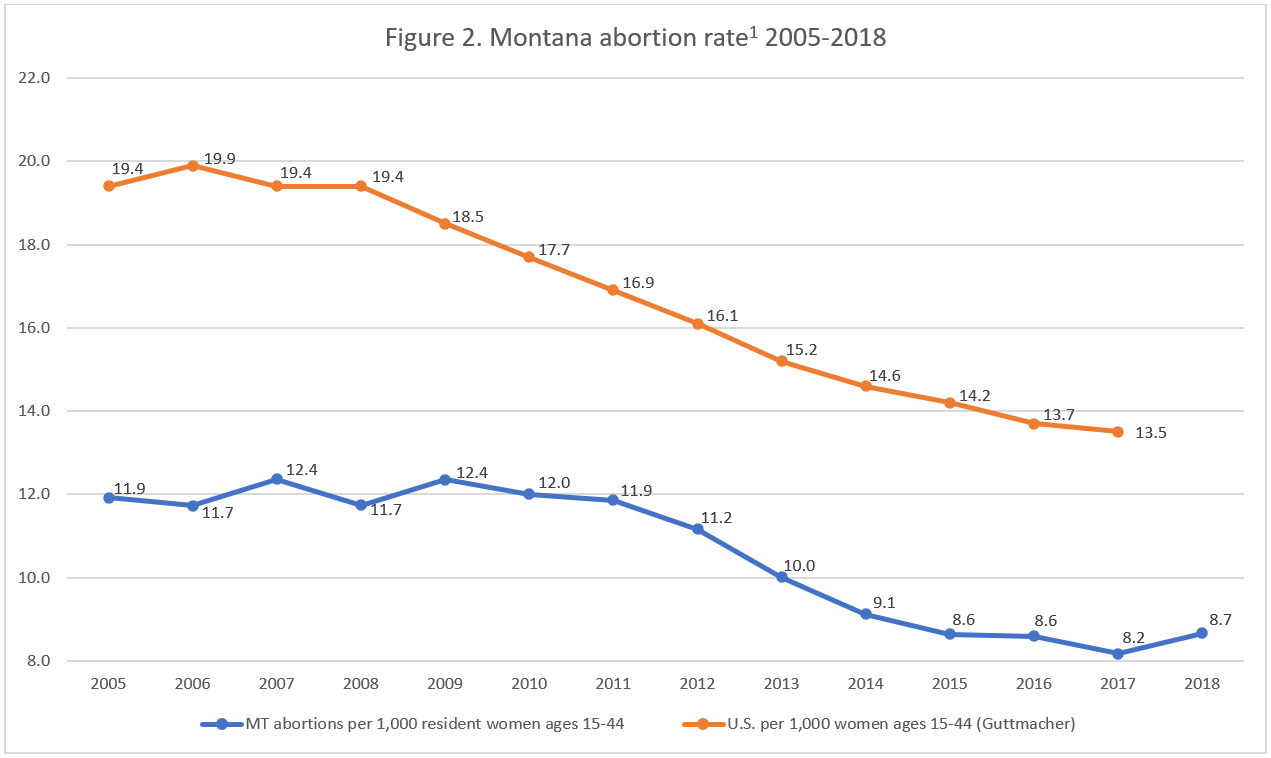
- Starting with the 2018 abortion reports, abortion rates are calculated by the Charlotte Lozier Institute to allow for easier state-to-state and year-to-year comparisons. Rates were calculated by CLI using population estimates from the United States Census Bureau. The rates were calculated using the following formula: (total number of abortions performed in Montana ÷ number of resident women ages 15-44) x 1,000. Rates may differ slightly from previous CLI articles due to revised population estimates.
Click here to view reporting from:2023202220212020201920172016















