











Editor’s Note: This paper was updated on June 27, 2025 to reflect changes made to #WeCount’s data limitations section in its most recently released report.
This is Issue 34 of the American Reports Series.
Appendix A (Table 1), Appendix B (Tables 2-7), Appendix C (Table 8), and Appendix D (Table 9), referenced throughout this paper, can be found here.
Executive Summary
- This paper provides, for the first time, a holistic overview of abortion provision in post-Dobbs America. No other paper has systematically collected point-in-time totals for the different types of abortionists as this paper has, nor has one examined, in depth, which estimates are the most complete and definitive.
- The most accurate, current, and complete data shows that 1,121,450 abortions were performed within the formal U.S. health care system from July 2023 to June 2024. Peer-reviewed research also shows thousands upon thousands of self-managed drug-induced abortions occurring outside the formal health care system.
- As of February 2025, surgical and/or drug-induced abortions were performed at 777 brick-and-mortar centers across America, while mail-order, drug-induced abortions were accessible through 142 different U.S.-based organizations or centers, and 8 websites or organizations operating outside the formal U.S. health care system.
- There is no federal mandatory abortion reporting requirement in the United States and only pro-abortion organizations are provided data from abortion centers. This leaves other research groups to only observe and analyze data from third parties instead of having access to the same raw data as pro-abortion organizations.
Introduction
The Dobbs decision in June 2022 fundamentally changed the abortion policy landscape in America. As a result of that landmark Supreme Court decision, many states were able to enact laws prohibiting abortion at conception or different gestational ages. However, while pro-life states acted quickly to enact these laws, pro-abortion states moved almost as quickly to shore up a “constitutional right” to abortion at the state level and enact policies that circumvent pro-life laws in other states. Data has shown that while pro-life laws are preventing brick-and-mortar abortions from occurring in pro-life states (and that is to be commended), the aforementioned strategies of pro-abortion states are proving to, in certain ways, counteract those pro-life laws. Furthermore, the abortion industry’s adaptations in strategy have exposed flaws in the construction of state pro-life laws. The pro-abortion Guttmacher Institute’s Monthly Abortion Provision Study estimated that over one million abortions occurred in the United States in 2023.[1] Additionally, more abortions occurred in 2023 than in 2020 (an increase of 11%). How could this happen after a Supreme Court decision allowing over 10 states to enact laws intended to protect life at conception?
In theory, the Dobbs decision should have decreased the total number of U.S. abortions. After the decision, Texas, a previously high abortion-volume state, no longer permitted the performance of abortion at brick-and-mortar centers except in cases where a continued pregnancy threatened the mother’s life and/or physical health.[2] Other higher-volume states such as Tennessee[3] and Indiana[4] implemented similar laws. Preliminary data suggested that abortions occurring within the formal health care system did in fact decrease in the last months of 2022 after the Dobbs decision.[5] However, the average monthly decreases were quickly erased in 2023 and beyond. A media report similarly noted that enough abortion drugs had been ordered from other countries to neutralize and even counteract the brief decline in abortions reported in 2022.[6] The hypothesis that total abortions would inevitably decrease post-Dobbs did not account for the questionable legal strategies pro-abortion states were willing to implement which only exposed and exploited loopholes in pro-life laws. From taking advantage of the FDA’s pre-Dobbs decision to allow mail-order telehealth abortions with no in-person requirement, to shipping abortion drugs into pro-life states from pro-abortion states under shield laws, to deeming certain states “abortion havens,”[7] pro-abortion states have circumvented the inability of women in pro-life states to obtain brick-and-mortar abortions.[8]
How many abortions have occurred post-Dobbs?[9] Researchers cannot give the public a single, definitive, and exact answer. This is partly because the United States lacks a federal abortion reporting requirement. An exact answer is also impossible to arrive at because state health departments tasked with collecting such data claim to be unable to track abortion drugs being shipped into their states or the number of women from pro-life states who travel out of state to obtain abortions.[10] While no definitive answer to the above question exists, organizations such as the Guttmacher Institute and the Society of Family Planning’s (SFP) #WeCount project have designed mathematical models and survey techniques to estimate the rounded number of abortions occurring at the state and national levels within the formal health care system. A third reason researchers cannot calculate the precise number of U.S. abortions, however, is that the number of abortions occurring outside the formal health care system is unknown.
This paper will not try to suggest numbers that differ from, or attempt to disprove, Guttmacher’s or SFP’s estimates. Charlotte Lozier Institute cannot do so because only pro-abortion organizations get access to center-level data. Instead, for the first time post-Dobbs, a holistic overview of abortion provision in post-Dobbs America will be laid out as well as a literature review of the different estimated abortion totals in 2023 and 2024 No other paper has systematically collected point-in-time totals for the different types of abortionists as this paper has, nor has one examined, in depth, which estimates are the most complete and definitive. This paper will also describe a variety of general estimates related to the number of abortions occurring outside the formal health care system. The last part of this paper will offer two clarifications regarding current narratives surrounding post-Dobbs abortion data using other Guttmacher and #WeCount data points in a way that contributes novel analysis that neither Guttmacher nor SFP has offered thus far.
Recent abortion totals will be discussed in two ways: by type of provider and by year. The most accurate, current, and complete statement regarding post-Dobbs abortion totals in the United States draws from data released by SFP. This data shows that 1,121,450 abortions were performed within the formal U.S. health care system from July 2023 to June 2024. In addition to the abortions occurring within the formal health care system, peer-reviewed research shows thousands upon thousands of self-managed drug-induced abortions occurring outside the formal health care system.
Appendix A (Table 1), Appendix B (Tables 2-7), Appendix C (Table 8), and Appendix D (Table 9), referenced throughout this paper, can be found here.
Three Recent Regulatory and Legal Changes that Have Impacted Abortion Provision
Before detailing how Guttmacher, SFP, and individual researchers arrived at their various estimates, it is critical to briefly summarize the changes that have allowed for an influx of abortion drugs being sent into pro-life states, the traveling of women from pro-life states to pro-abortion states, as well as the increase in resident women obtaining abortions in pro-abortion states.
Telehealth Abortions
Even before Dobbs, mail-order, telehealth abortions were increasing within the formal health care system. In 2020, the United States Food and Drug Administration (FDA) temporarily stopped enforcing mifepristone’s in-person dispensing requirement.[11] This change was made official in December 2021.[12] In January 2023, the agency removed the in-person dispensing requirement from the regulatory rulebook for mifepristone.[13] These changes to the drug’s Risk Evaluation and Mitigation Strategy (REMS) allowed brick-and-mortar abortion centers to dispense mifepristone via the mail. Moreover, the FDA’s decisions lead to the creation and proliferation of virtual centers that send abortion drugs around the country.
Due to these regulatory changes, telehealth abortions have become an increasing percentage of the total number of U.S. abortions. According to one #WeCount report, while the total number of abortions decreased from April 2022 to December 2022, the number of telehealth abortions increased from 4% to 11% of all abortions during that same period.[14] More recent data found that telehealth abortions accounted for 16% of nationwide abortions in September 2023,[15] while #WeCount’s most recent data showed a 155% increase in the number of telehealth abortions from the second quarter of 2023 to the second quarter of 2024.[16] That same report noted that as of the second quarter of 2024, telehealth abortions accounted for 20% of the nation’s abortions. No regulatory changes or previously existing laws ever allowed for the importation of mail-order abortion drugs from overseas (outside the formal health care system) or mailing abortion drugs within the formal health care system. However, the laws prohibiting the mailing of abortion drugs are not being enforced.[17]
The Dobbs Decision
The Dobbs decision undoubtedly had one of the biggest effects on the changes to abortion provision in America. As a result of the decision, the legality of abortion changed dramatically across the country. State and federal legislatures were now free to enact policies that would protect the unborn from the moment of conception or other pre-viability gestational ages. As of February 2025, 12 states prohibit abortion except in limited cases.[18] Abortion is prohibited after a baby’s heartbeat can be detected in four states and at different gestational points before “viability” in another four states.[19] It is important to clarify that in such states the law prohibits abortions performed at brick-and-mortar centers, but they do not make it illegal for women to obtain abortion drugs from abortionists in other states or travel to other states to obtain an abortion. Apart from these changes to states’ gestational laws, several states had enacted telemedicine restrictions before Dobbs or have since. In states where abortion is still legal at some point, telemedicine abortions are prohibited or restricted in 12 states.[20]
As some states moved to protect unborn children after the Dobbs decision, others passed ballot amendments to enshrine the “right” to an abortion in their state constitutions.[21] Additionally, at the time of the Dobbs decision, nine states already had post-viability abortion restrictions that do not in practice substantially protect the unborn because of the laws’ broad exceptions. These laws remain in effect.[22] Another nine states and the District of Columbia (D.C.) have no limits on when an abortion can be performed.[23] As data described in the proceeding sections will show, the states where abortion is legal throughout pregnancy or widely unrestricted are compensating for the decline in abortions performed in brick-and-mortar facilities in states that have since prohibited or restricted the performance of brick-and-mortar abortions.
Shield Laws
The invention and implementation of shield laws have also profoundly impacted the increase in access to abortion since Dobbs. Shield laws protect abortionists from various forms of legal and professional liability who provide abortion drugs to or perform surgical abortions on women from other states that prohibit or restrict abortion.[24] This can include, for example, immunity from criminal, civil, and malpractice consequences; states declining to enforce judgments against abortionists issued in pro-life states; and rejecting the application of pro-life laws in the shielding state’s courts (among other provisions).[25]
What differentiates certain shield laws is whether the law shields both abortionists who ship abortion drugs into pro-life states after conducting a telehealth consultation and also those providing drug-induced and/or surgical abortions to out-of-state women within the shielding state, or whether the law instead only shields the latter. Fourteen states and D.C. have the latter type of shield law (shielding only abortionists providing in-state abortions to out-of-state women).[26] Eight states have enacted the former type of shield law; laws that both protect abortionists providing in-state abortions to out-of-state women as well as those in shielding states who send abortion drugs to states that either prohibit or restrict brick-and-mortar or telehealth abortions.[27]
The Different Modes of Abortion Provision: Brick-and-Mortar Centers or Mail-Order Abortions
Abortions Performed at Brick-and-Mortar Centers
Before telehealth abortions were legally permitted and prevalent, many associated abortion primarily with in-person surgical or drug-induced abortions performed at brick-and-mortar abortion centers. While telehealth abortions are increasing rapidly, a majority of abortions in the United States are still performed at brick-and-mortar centers.[28] Currently, there are 777 such centers in the United States with 454 providing both drug-induced and surgical abortions, 319 providing only drug-induced abortions, and four providing only surgical abortions. Brick-and-mortar abortion centers include Planned Parenthood centers, independent centers, mobile centers, and hospitals/doctors’ offices.[29] To see the number of brick-and-mortar centers by state, see Table 1 in Appendix A.
Mail-Order Abortions
The other mode of abortion provision is mail-order abortion. For this type of abortion, women do not have to go to an in-person appointment at an abortion center or doctor’s office to get the abortion drug regimen (mifepristone and/or misoprostol). The exact logistics of a mail-order abortion depend on whether the abortion is occurring in or outside the formal U.S. health care system, and if within the formal health care system, on the specific organization/center a woman is requesting abortion drugs from. There are four main types of mail-order abortion providers: online-only centers and organizations, hybrid brick-and-mortar online centers, online e-commerce websites that sell abortion drugs, and community network support groups. In the following paragraphs, these four types of providers will be described more in-depth. For more details on the different organizations/centers associated with this type of abortion provision, see Tables 2-7 in Appendix B.[30]
Online-only centers and organizations (hereafter ‘OOCOs’) operate domestically and internationally. U.S. OOCOs operate within the formal health care system and use telehealth platforms to prescribe women abortion drugs. The protocol for U.S.-based OOCOs is typically as follows[31]: First, the abortionists associated with the OOCO review the woman’s medical intake form. Sometimes the abortionists will be required to consult with the woman via a telehealth platform, or voluntarily do so, depending on the requirements and protocol of the specific organization or center. If the woman is deemed eligible to take the drugs, the provider will send a prescription for the regimen to a partnering pharmacy. The pharmacy then ships the abortion drugs directly to the woman. Whether the OOCO provides women with follow-up support or the opportunity to correspond with the abortionist varies.
There are two different types of U.S. OOCO: organizations that ship abortion drugs to women in all U.S. states under the protection of one of the eight existing shield laws and centers/organizations that ship abortion drugs to women only in certain U.S. states. There are currently four organizations that ship abortion drugs to all U.S. states under shield laws. Aid Access is by far the biggest distributor of abortion drugs to women in states where brick-and-mortar abortions are prohibited.[32] The abortionists who partner with these four organizations operate under one or more of the eight shield laws and must be licensed to practice medicine in the shielding state. Women can complete the telehealth appointment from a state where brick-and-mortar abortions are prohibited and have the drugs shipped directly to their residences. Relatedly, 37 OOCOs ship abortion drugs to women only in certain states[33] where abortion remains legal, but which states they ship to varies for each one. It is important to note that these 37 OOCOs do not require women to be residents of the states they ship the drugs to or remain in the state to take the abortion drug regimen.[34] They only require that the women be physically present in a state the organizations ship to at the time of the telehealth appointment and have a mailing address in the state where the abortionist is licensed to practice. These companies allow women to have the drugs shipped to someone else if they are helping the woman obtain the drugs.
Many organizations/centers also offer the advanced provision of abortion drugs to those who want to have a drug-induced abortion in the future. To see which centers and organizations offer the advanced provision of abortion drugs, see Tables 2-4 in Appendix B.
A subtype of U.S. mail-order telehealth organizations/centers is the brick-and-mortar centers that also offer telehealth abortion services. Often called “hybrid” centers, these centers have a physical location that performs in-person surgical and/or drug-induced abortions while also mailing abortion drugs to women within the state in which the center is located via telehealth. To see the number of U.S.-based mail-order, telehealth organizations that ship to a specific state as well as the number of hybrid brick-and-mortar centers by state, see Table 8 in Appendix C. To see more generalized information about hybrid organizations and centers, see Table 4 in Appendix B. Hybrid centers were categorized separately from U.S. online-only organizations/centers because hybrid entities have a physical location and an online presence. However, telehealth abortions performed by hybrid centers follow virtually the same protocol as the U.S. online-only centers/organizations.
In addition to U.S. online-only and hybrid centers/organizations, there are international online organizations that operate outside the formal U.S. health care system. Three organizations operate outside of the U.S. but mail abortion drugs into the country using abortionists licensed in other countries. These organizations utilize virtually the same protocol as the U.S. online-only organizations but the drugs being sent to women are not FDA-approved. Furthermore, they do not use telehealth platforms licensed for use in the United States. To see a description of these three organizations, see Table 5 in Appendix B.
Along with international organizations, there are online, typically foreign websites that sell abortion drugs to women in any U.S. state and operate outside the formal U.S. health care system. These are e-commerce websites that provide no physician support to women if they have post-abortive complications or follow-up questions. Additionally, they do not require a woman to complete an intake form or verify how far along she is in her pregnancy. At least three e-commerce websites ship abortion drugs into the United States.[35] These websites, as well as international organizations, rely on the bulk production and distribution of abortion drugs in different countries around the world.[36] The different online websites sell drugs manufactured in foreign countries and then ship bulk orders to different supply chain sources in the United States who then ship the drugs to women.
The last variation of mail-order abortion providers operating outside of the formal health care system is community network support groups. These groups are composed of community-based distributors who supply women around the U.S. with free abortion drugs, relying on suppliers who obtain privately donated drugs or drugs from international pharmacies at a cheap price.[37] Volunteers then receive and distribute the drugs to women across the country. Women can either have volunteers working with the community network support groups mail them the abortion drugs or meet up with women so they can pick them up in person. Women who request abortion drugs from these groups are not required to have a prescription and the groups do not provide any physician support if women experience post-abortive complications or have questions. The focus of these groups is to provide abortion drugs to women in states where abortion is prohibited or restricted after 6 to 12 weeks.[38] To see the overall breakdown of abortion provision in the U.S. graphically, see Figure 1 below.
Figure 1 – The Different Modes of Abortion Provision in the United States

Who Reports What? How Abortion Data is Reported in the United States
To properly understand abortion estimates in the U.S. it is critical to first understand how those estimates get reported (or don’t get reported). There is no federal mandatory abortion reporting requirement in the United States. Because of this, the only federally produced abortion data is voluntarily submitted to the Centers for Disease Control (CDC) by select states.[39] The CDC then publishes the data on a delayed schedule in its abortion surveillance summaries. Due to how incomplete and delayed the CDC’s data is, the agency’s 2022 abortion data contained within its annual abortion surveillance reports was not used in this paper. In addition to the voluntary CDC data, 47 reporting areas are required by state law to release online annual abortion reports or provide them to the public upon request.[40] These reports vary in quality and timeliness.[41] No state-published reports include the number of abortions occurring outside the formal health care system and most do not include telehealth abortions occurring in and outside of their states within the formal health care system.[42] Because of the incompleteness and varying degrees of timeliness associated with state-published data, state abortion data were not used in this paper.
Apart from public sector reporting (or non-reporting) entities, the private pro-abortion organizations Guttmacher and SFP publish state and national abortion totals, as well. Initially, Guttmacher released state abortion estimates through its Abortion Provider Census using data collected from the survey results of 1,603 abortion centers. According to the most recent Census report, an estimated 930,160 abortions were performed across the country in 2020.[43] This total, unlike the CDC and state reports, includes estimated totals for states that do not publish abortion data. After Dobbs, Guttmacher started a new initiative, the Monthly Abortion Provision Study.[44] This initiative collects state-level monthly abortion estimates (from January 2023 through November 2024).[45] Guttmacher gets these totals from a combination of monthly surveys from a sample of abortionists and statistical modeling that uses historical abortion caseloads from providers around the country to impute missing data. The initiative collects abortion totals in states where abortion is still legal at some point but does not include monthly estimates for states that prohibit the performance of brick-and-mortar abortions.[46] Guttmacher’s initiative also collects data on how many women are obtaining abortions in their states of residence and how many are traveling out of state to obtain abortions in states where brick-and-mortar (surgical or drug-induced) abortions are still legal. Lastly, Guttmacher compares the data it collected for 2023 with 2020 totals to show how Dobbs changed U.S. abortion access.
In Guttmacher’s Monthly Abortion Provision Study, abortions are counted as having been performed in the state where women obtained a surgical or drug-induced abortion, or where abortion drugs were dispensed to, regardless of whether the woman obtained the abortion in her state of residence or traveled to get the abortion. Unlike many states’ reporting systems, this initiative can capture telehealth abortions performed by online-only centers/organizations and hybrid brick-and-mortar centers in states where telehealth abortions are still legal. While Guttmacher’s totals are not as complete as #WeCount’s, Guttmacher’s data was still used to calculate other data points used throughout this paper as the study includes data related to topics not touched on by #WeCount reports. The last formal source of abortion data in the United States is from SFP’s #WeCount project. Like Guttmacher’s initiative, the #WeCount project reports monthly abortion totals, but unlike Guttmacher, #WeCount’s data includes abortion totals for every state. #WeCount’s data even includes estimates for states where brick-and-mortar abortions are prohibited but women obtain abortion drugs under shield laws.[47] SFP has data on abortion totals from April 2022 to June 2024. #WeCount surveys all abortionists in the country and when they don’t receive data from abortionists, they impute data using the data published by states’ health departments. The most recent report was released in October 2024.[48] The totals within this report include surgical and drug-induced abortions performed in person at brick-and-mortar centers as well as drug-induced telehealth abortions performed via online-only centers/organizations and hybrid brick-and-mortar centers. All abortions reported by #WeCount, including telehealth abortions, are counted according to the state where the abortion was performed, or the abortion drugs were mailed to. In July 2023, SFP’s reports started further breaking down telehealth abortion totals by those performed by hybrid brick-and-mortar centers and those performed by online-only centers/organizations. The inclusion of shield law data is why CLI used #WeCount estimates to inform the main estimates described in this paper.[49]
An important caveat when discussing the number of abortion drugs mailed by different organizations/centers is that the number of drugs mailed is not necessarily equal to the number of abortion drugs taken by the women they are sent to or the number of completed abortions. Similarly, the number of abortion drugs requested by women is not necessarily equal to the number of abortion drugs mailed, as an abortionist may deem a woman ineligible for a telehealth abortion because of how far along she is in her pregnancy or other clinical reasons.
No private or public U.S. reporting entity tracks and reports the number of self-managed abortions. To give readers a general estimate of the number of abortions obtained outside the formal health care system, CLI will provide a variety of estimates from different peer-reviewed sources and news articles as well as simple calculations that take drug usage rates into account.
Similarly, no reporting entity details the number of abortion drugs provided via advanced provision. CLI will briefly summarize the one study that estimates the number of requests for the advanced provision of abortion drugs. No studies detailing the actual number of drugs mailed via advanced provision exist in the current literature. Relatedly, there are no estimates of the number of abortion drugs provided under advanced provisions that result in a future completed abortion. However, data on the number of drugs requested through advanced provision is still helpful to know the demand for abortion drugs in a pre- and post-Dobbs country.
How Many Abortions Have Occurred in America – By Type of Abortion Provider
The most recent and complete total number of abortions occurring in America (1,121,450) is from the #WeCount project, utilizes data from July 2023 to June 2024, and can be broken down by the types of abortionist within the formal U.S. health care system. This yearly total and the totals by type of provider that comprise it are the most accurate estimates available to the public and represent the results of the most current policy landscape.
Figure 2 – Total Number of Abortions by Type of Provider, July 2023 – June 2024
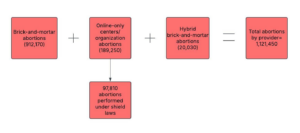
These totals were calculated using Tables 2-2023B, 2-2024A, 3-2023 Q3-4, and 3-2024 Q1-2 in the October 2024 #WeCount report.[50] The total for abortions provided under shield laws was calculated using those same tables and included abortion drugs sent to women in states where brick-and-mortar abortions were prohibited throughout pregnancy, after six weeks of pregnancy, and to women in states where there are telehealth abortion restrictions or prohibitions.
As a result of the proliferation of the different types of mail-order abortion providers (especially ones within the formal health care system), and much of the media attention on this type of abortion, it is important to note that a statistically large majority of abortions in America for which researchers have data are occurring at brick-and-mortar centers. In Figure 3, one can see that abortions performed at brick-and-mortar centers accounted for 81% of the abortions performed from July 2023 to June 2024, a time when the usage of telemedicine for abortion was at an all-time high. Nineteen percent is not a statistically insignificant percentage for the number of abortions being performed via telehealth, especially since that figure was 4% less than three years ago. The rapid growth in the percentage of abortions being performed via telehealth is not to be understated. From a public health perspective, however, it is equally important to portray how much demand there still is for in-person abortions as different demographics of women seek in-person versus telehealth abortions.[51] If the pro-life movement wants to effectively address both the supply and demand for the two different types of abortion occurring within the formal U.S. health care system, it should understand the full picture. To see the graphical breakdown of abortion provision within the formal U.S. health care system over a year, see Figure 3 below.
Figure 3 – Percentage Breakdown of Abortions by Type of Provider within the Formal Health Care System, July 2023 – June 2024
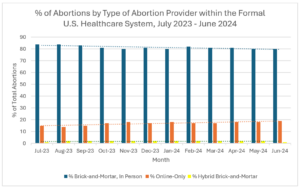
From a statistical perspective, it is interesting that the trendline for each type of provider does not significantly change over a year. This suggests that while there was an initial significant increase in the percentage of abortions performed by telehealth providers after FDA changes and the Dobbs decision, the increase leveled off a little over a year after the Supreme Court decision.[52] This is not to say that the number of telehealth abortions will not continue to increase, but rather that the percentage breakdown of abortions by type of provider seems stable for now. The increase in one type of abortion provision does not necessarily mean that another type of provision will decrease. Brick-and-mortar centers also provide abortion drugs, so when it is noted above that telehealth provision has seemed to level off in a way, the percentage of abortions performed with abortion drugs continues to increase. Guttmacher noted that in 2023, 63% of all abortions obtained by women in states without total prohibitions on brick-and-mortar abortions were drug-induced.[53]
As previously mentioned, no formalized data collection or reporting process exists for abortions performed outside of the formal U.S. health care system. Because of this, CLI gathered very rough estimates for the number of abortion drugs mailed by the different modes of mail-order abortion provision that occur outside of the formal health care system from different peer-reviewed publications and a news article. Furthermore, because the number of abortion drugs mailed by a provider doesn’t necessarily equal the number of abortion drugs taken or the number of completed abortions, it was necessary to find scholarship on the usage rates for the different modes of self-managed abortions; in other words, what percentage of women take the abortion drugs mailed to them. One such study (Aiken et al., Mar 2024) satisfied both CLI’s search for rough estimates and usage rates.[54] The study’s authors reached out to all existing providers outside of the formal health care system at the time of the study and inquired about the estimated number of abortion drugs the organizations mailed out during the study period. The authors ultimately received estimates from 15 unique sources and 28 sub-sources. The authors also reviewed the existing literature to give average estimated usage rates for the different modes of abortion-drug provision related to self-managed abortions. Given the estimates reported in the study along with the corresponding usage rates, the estimated number of self-managed abortions were as follows for July – December 2022:[55]
Table 10 – Estimated Number of Mail-Order Drugs Mailed and Taken Per Abortion Drug Provider Operating Outside of the Formal U.S. Health care System[56]
| Actual # of abortion drugs mailed out, July - December 2022 | Usage Rate (%) | Estimated # of Abortion Drugs Taken by the Women Requesting the Drugs (Rounded to the Nearest Tens Place) | |
| Community Networks | 18,321 | 98.5% | 18,046 |
| Online websites* | 6,919 | 86%** | 5,950 |
| International telehealth organizations | 13,223 | 88% | 11,640 |
| Total | 38,463 | - | 35,636 |
* 2,876 of the 6,919 total abortions for this mode of provision were imputed by the authors from additional online websites that didn’t respond to the authors’ study questions.
** No literature existed on the average usage rate of abortion drugs sold by online websites, so the study’s authors used the lowest published usage rate from the four studies found in footnote 38 for telehealth organizations as they believed that online websites were more similar in operation to international telehealth organizations than community networks.
In addition to Aiken et al.’s 2024 research on the supply of self-managed abortion drugs post-Dobbs, another similar peer-reviewed article details the demand for such drugs (Aiken et. al, 2022).[59] The article lists the mean number of requests for abortion drugs from Aid Access during three time periods in 30 states where Aid Access was not yet operating within the formal health care system:
- A pre-Dobbs baseline period: 9/1/21 – 5/1/22 – 6 mean daily requests
- After the Dobbs decision was leaked but before the formal ruling: 5/2/22 – 6/23/22 – 1 mean daily requests
- After the Dobbs decision was released: 6/24/22 – 8/31/22 – 7 mean daily requests
In a New York Times article, Aiken, the principal author of both peer-reviewed articles just described, noted that 50-60% of women who submit requests to Aid Access receive abortion drugs.[60] If an average percentage of 55% was applied to the mean number of post-Dobbs daily requests for abortion drugs, around 118 requests would result in shipments per day in a roughly two-month period. Because the authors noted several study limitations, it is best to not extrapolate this data to calculate mean daily request totals for other months and years. However, the rough estimates presented above can be used as a minimum benchmark when thinking about one type of abortion drug provider that (previously) operated outside of the formal health care system.
Other than the two studies described above, there is a paucity of peer-reviewed research on the number of self-managed abortions in post-Dobbs America in large part because of how hard it is to track not just the number of abortion drugs sent by differing providers, but the number of abortions drugs taken by women. Considering this lack of research, researchers largely depend on media reports on the number of abortion drugs mailed out from international online websites, online websites, and community network support groups. While the following table in no way contains a complete list of available estimates published by the media, it does contain a sample of estimates from the previously mentioned NYT article in which several different types of abortion-drug providers were interviewed that operate outside of the formal U.S. health care system as of April 2023. Because not all abortion drugs requested result in abortion drugs being shipped or eventually taken, these estimates provide an extremely broad overview of self-managed abortions post-Dobbs:
Table 11 – Estimated Number of Mail-Order Drugs Requested or Sent Per Abortion Drug Provider Operating Outside of the Formal U.S. Health care System[61]
| Where the Abortion Drugs are Coming From | Measurement | Estimated # of Abortion Drugs |
| Overseas abortion drug suppliers that provide the 3 types of “informal” abortion drug providers with abortion drugs | Projected # of abortion drugs sent to women in the United States in 2023 by overseas suppliers via organizations/websites operating outside the formal health care system | Abortion drugs sent to 100,000 people* |
| Online website (unnamed) | # of abortion drug orders distributed in two weeks in February 2023 | 300 |
| Aid Access (when it was strictly an international online organization and not part of the formal U.S. health care system) | How many abortion drugs were provided to women seeking to obtain abortion drugs outside the formal health care system from July - December 2022 | Around 23,000. Aid Access told the authors of this article that 50 to 60% of orders result in shipments, and the 23,000 figure reflects this estimate. |
| Las Libres | How many abortion drugs were requested by women seeking to obtain abortion drugs outside the formal health care system from July - December 2022 | Around 17,500 |
| Online websites | How many abortion drugs were requested by women seeking to obtain abortion drugs outside the formal health care system from July - December 2022 | Around 9,500 |
| Private Emma | # of abortion drug “kits” sent to U.S. women per month | 5,000 |
* The article didn’t specify the number of pills sent in the drug regimens mailed to women so the total number of women receiving drugs was included instead.
WeCount’s figure for total abortions considers the number of abortions performed under shield laws and provides researchers with an insight into the total number of abortions during this time period by type of provider, while the broad statement of “thousands upon thousands” of self-managed abortions is as complete as the existing data allows researchers to make for that type of abortion provision.
Only one peer-reviewed article even attempted to estimate a number associated with the advanced provision of abortion drugs post-Dobbs. A January 2024 study written by Aiken et. al described the estimated demand for the advanced provision of abortion drugs from Aid Access in all 50 states and D.C. during four different periods.[63] These periods and their corresponding mean daily requests include:
- A pre-Dobbs baseline period: 9/1/21 – 5/1/22 – 8 mean daily requests
- After the Dobbs decision was leaked but before the formal ruling: 5/2/22 – 6/23/22 – 3 mean daily requests
- After the Dobbs decision was released: 6/24/22 – 4/6/23 – 1 mean daily requests
- During conflicting judicial rulings on the FDA REMS approval for mifepristone: 4/7/23 – 4/30/23 – 1 mean daily requests
In total, during the entirety of the study period (9/1/2021 – 4/30/2023) and when Aid Access was operating outside of the formal health care system, Aid Access received 48,404 total requests for advanced provision. The study found that after the leak and the Dobbs decision itself, the mean daily request rate was highest in states where brick-and-mortar abortions were likely to be prohibited in the future.
How Many Abortions Have Occurred in America, By Year
While considering the total number of abortions performed from July 2023 through June 2024 is helpful when looking for the most recent and complete United States abortion data, it is also informative to look at the number of abortions occurring in other periods throughout 2023 and through October 2024. Because abortion access and provision are influenced by legal changes that happen across periods, monthly and yearly data are critical to researchers’ understanding of how policies impact human behavior and subsequent abortion totals. The data from #WeCount and Guttmacher’s Monthly Abortion Provision Study both capture abortions in their places of occurrence (where surgical abortions are occurring and where abortion drugs are mailed). However, because only #WeCount’s data incorporates abortion drugs being mailed and taken by women in states (under shield laws) where brick-and-mortar abortions are prohibited, the following Guttmacher totals are slightly lower than #WeCount’s. Furthermore, while #WeCount’s data is the most complete available, even their pre-July 2023 monthly numbers are an undercount and make totals including those months undercounts as SFP did not start counting abortions performed under shield laws until July 2023. Below are various monthly and yearly totals calculated using various tables from #WeCount and Guttmacher’s data:
Table 12 – Monthly and Yearly Totals from #WeCount and Guttmacher Data, 2023 – October 2024[64]
| #WeCount’s Estimate | Guttmacher’s Estimate | |
| 2023 | 1,056,150 | 1,032,140 |
| Jan - June 2024 | 587,440 | 543,780 |
| Jan - October 2024 | Not available yet | 878,090 |
| 2023 - June 2024 | 1,643,590 | 1,575,920 |
| 2023 - October 2024 | Not available yet | 1,910,230 |
| July 2023 - June 2024 | 1,121,450 | 1,053,850 |
The fact that #WeCount’s and then Guttmacher’s data is the most accurate and complete data available does not mean it is without flaws. One of the biggest weaknesses with both projects’ data is the lack of reproducibility. No one except pro-abortion organizations like SFP and Guttmacher gets access to totals reported by centers and organizations themselves, and the two organizations do not publish raw totals by organization or center. Consequently, there is no way to reproduce or confirm the validity of the report data, a common feature of social science data. Lastly, while one might suspect that the ideologies of the organizations putting forth these data and conclusions are scientifically and morally wrong, the data, statistically speaking, is the best researchers have.
Two Clarifications Regarding post-Dobbs Data
Many of the post-Dobbs national conversations regarding abortion have focused on the increase in abortions following the decision. This section will seek to clarify two points regarding post-Dobbs data that are often highlighted in the media.
Clarification #1 – The Truth About Where and How American Women Are Obtaining Abortions
In a post-Dobbs America, there has been a large focus by the media and academia on the impact that the decision has had on changes to where and how women are obtaining abortions. The media has seized this opportunity to highlight the number of women from states with brick-and-mortar abortion prohibitions utilizing other states’ shield laws and traveling to other states to obtain abortions. What is often not talked about in as great of detail, or at all, is the fact that a majority of abortions contributing to the overall increase are obtained in states where abortion remains largely legal by residents of those states. Articles such as an NPR piece from May 2024 do not mention this important fact in their discussion of the increase in abortions.[65] Even the organizations responsible for disseminating the data used in this paper bury this subtle but important caveat deep in their analyses of their data while publishing attention-grabbing headlines about abortion “bans.”[66]
Any article discussing post-Dobbs abortion data should note that a large number of abortions have been obtained under shield laws by women from states that now prohibit brick-and-mortar abortions. There is no hiding the impact that shield laws have had on the overall nationwide increase in abortions post-Dobbs. As noted in Figure 2, 97,810 abortions occurred under shield laws from July 2023 to June 2024 (9% of the total number of abortions in that period). That number is not statistically insignificant, especially since it means that 97,810 unborn children were killed by abortion. However, it is equally important to note that 1,023,640 (or 91%) of the 1,121,450 total abortions that occurred during that timeframe were not obtained under shield laws. This means that more abortions occurred in the smaller number of states where abortion is still legal in the period from July 2023 to June 2024 than occurred in all of 2020 when brick-and-mortar abortions were legal in every state (930,160). Even using a slightly lower total number of abortions for the July 2023 – June 2024 period from Guttmacher (1,052,850) yields a number (958,093) of abortions (not performed under shield laws) higher than the number of abortions performed in 2020.
Relatedly, the data shows that there has been a substantial increase in the number of women who traveled from their states of residence to other states to obtain abortions from 2020 to 2023. Guttmacher’s 2023 data showed that 168,630 women traveled out of their state of residence to obtain an abortion.[67] The number of women who traveled out of state more than doubled from 2020 when 74,470 women traveled out of state to get an abortion: 9% of the 2020 total. Of those 168,630 women, 98,690 were from states where brick-and-mortar abortions are prohibited, 30,740 women were from states where abortion is restricted, and 39,200 women were from states where abortion remains widely available and legal.[68] However, abortions obtained by out-of-state residents from pro-life states are not solely, or even primarily responsible for the majority of abortions occurring in 2023 nor the nationwide increase in the number of abortions occurring post-Dobbs. If 168,630 (16%) women traveled to get an abortion in 2023, that means 860,610 (84%) abortions were performed on state residents in states where abortion was still legal.
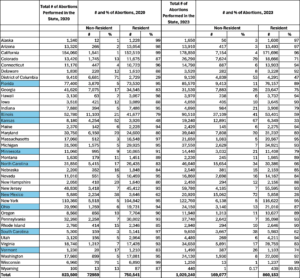
In the U.S. there were 38 areas (37 states and D.C.) where abortion was legal for some or all of 2023. An analysis of Guttmacher data shows that in 34 of the 38 states/areas, abortions increased from 2020 and in four areas (three states and D.C.) abortions decreased. In 21 of the 34 states where abortions increased, the increase in resident abortions was more responsible for the increase in overall abortions than the overall increase in nonresident abortions.[69] In four of the 34 states where abortions increased, resident abortions increased while non-resident abortions decreased, meaning the overall increase in abortions in 2023 was solely caused by the increase in resident abortions.[70] The nine states where the nonresident increase was more responsible for the state’s overall increase in abortions in 2023 include Florida, Illinois, Kansas, Minnesota, North Carolina, New Mexico, Ohio, South Carolina, and Vermont.[71] In 33 of the 38 areas where abortion was legal for some or all of 2023, nonresident abortions increased, while resident abortions increased in 34 areas. However, as the data shows, the majority of the increase in overall abortions in these states was caused by the increase in resident abortions. While the increase in nonresident abortions in 33 of the 38 states is not inconsequential, the increases in resident abortions were statistically more significant to the overall increase in abortions from 2020 to 2023 and the overall total number of abortions in 2023. See Table 13 for raw data.
Table 13 – Guttmacher’s 2020 and 2023 Residence Data[72]
The post-Dobbs adaptation in tactics by the abortion industry was partially responsible for the increase in abortions from 2020 to 2023 and the over one million abortions that occurred in the first full year post-Dobbs. The lack of a federal prohibition on abortions of any type (telehealth, in-person, etc.) at any gestational age also has been partially responsible for the over one million abortions occurring a year post-Dobbs in addition to the construction of pro-life laws. State laws and their effectiveness will be discussed next.
Clarification #2 – States with Pro-Life Laws Save Lives but are not ‘Abortion-Free’
In some of the states that have pro-life laws prohibiting brick-and-mortar abortions altogether or after six weeks, annual abortion reports have been released by state health departments claiming that zero abortions occurred in their respective states in 2023. These states include Arkansas,[73] Oklahoma,[74] and South Dakota.[75] While the reports are technically correct in that zero abortions were performed within their states at brick-and-mortar centers, all three reports fail to note that their state laws have not prevented abortions from occurring in their state via telehealth, that other states’ shield laws have allowed for telehealth abortions within their state lines, and that women are traveling out of state to obtain abortions. Even the states whose reports note the number of “abortions” performed under their states’ exceptions do not provide this information because the states do not collect this data.[76] The conclusion that states with pro-life laws in effect are now abortion-free should not be drawn from these reports. Data from #WeCount’s latest report showed that abortions increased in 10 of the 13 states where brick-and-mortar abortions were prohibited altogether or after six weeks for the entirety of 2023.[77] #WeCount used half of a year of data from the latter parts of 2023 and 2020 to show that the number of abortions obtained by resident women traveling to other states eclipsed the number of abortions obtained by women from those same states in 2020 when they obtained abortions at brick-and-mortar centers (either within or outside of their own states). The total number of abortions decreased from 2020 to 2023 in three states.[78] Overall, the data shows that during this time there was a net increase of 6,245 abortions among these 13 states. See the table below for a numerical breakdown.
Table 14 – #WeCount Abortion Totals for Six Months of 2020 and 2023 in 13 States with Pro-Life Laws in Effect for 2023[79]
| Abortion Total for Six Months of 2020 | Abortion Total for Six Months of 2023 | Difference | |
| Alabama | 4,460 | 5,115 | +655 |
| Arkansas | 2,220 | 2,250 | +30 |
| Idaho | 1,030 | 895 | -135 |
| Kentucky | 2,805 | 3,160 | +355 |
| Louisiana | 3,805 | 4,180 | +375 |
| Mississippi | 2,850 | 3,305 | +455 |
| Missouri | 5,795 | 6,580 | +785 |
| Oklahoma | 4,130 | 2,800 | -1,330 |
| South Dakota | 325 | 350 | +25 |
| Tennessee | 5,140 | 7,085 | +1,945 |
| Texas | 30,625 | 29,525 | -1,100 |
| West Virginia | 835 | 1,310 | +475 |
| Georgia | 18,115 | 21,825 | +3,710 |
| Total | 82,135 | 88,380 | Net increase of 6,245 |
The data described above shows a definitive increase in abortions in states that enacted pro-life laws post-Dobbs. Pro-life state laws are not written in a way that makes every means of abortion illegal and unattainable and are also subverted by the laws in pro-abortion states. However, this data should not be understood to mean that pro-life state laws did not prevent some abortions from occurring in these states. It is statistically and morally important to not discount the impact that pro-life laws are having on the number of brick-and-mortar abortions no longer occurring in several states; especially given the fact that most abortions are still performed at brick-and-mortar centers. In the most recent full year of pre-Dobbs Guttmacher data (2020),[80] 144,370 abortions were performed at brick-and-mortar locations within the 12 states that currently prohibit brick-and-mortar abortions. Objectors might argue that those women who can no longer get an abortion at a brick-and-mortar abortion in their states of residence can now travel across state lines or get the abortion drugs through the mail, potentially replacing a prevented brick-and-mortar abortion with a different type of abortion or an abortion in a different state. While this is true in some cases, it is not true in every case. Without data showing the individual decisions of women initially unable to obtain a brick-and-mortar abortions in their state of residence, this claim should not be made.
Current pro-life state laws do in fact act as a deterrent for some women seeking in-person abortions such as those who are further along in their pregnancy or who cannot logistically travel out of state to obtain an abortion. Furthermore, who is to say those brick-and-mortar abortions wouldn’t have happened in addition to (not instead of) the increasingly popular methods of obtaining abortions (traveling out of state, mail-order abortions, etc.)? The abortion industry would have most likely adopted some of the same changes to abortion access had Dobbs not occurred, perhaps at a different pace, but still adopted some of the changes, nonetheless. The abortion industry can only survive and thrive when abortion is widely accessible so it is not unreasonable to argue that the changes allowing for wider access to abortion would have occurred regardless of the Dobbs decision. After all, the total number of abortions was already increasing in large numbers before the Dobbs decision. According to Guttmacher’s 2020 abortion provider census study, abortions increased in from 2017 to 2020 by a total of 8%. Without the pro-life state laws, brick-and-mortar abortions could have occurred in addition to the abortions occurring via online-only organizations, hybrid brick-and-mortar centers, under shield laws, and/or outside the formal health care systems. The “prevented versus replaced” calculation is not linear. The statistics confirm two truths: pro-life laws are preventing some abortions but not enough to offset the increase in telehealth abortions, abortions occurring under shield laws, abortions obtained by women traveling out of state, or abortions obtained by residents of states where abortion is still legal.
Conclusion
What every data point in this paper describes, whether it be the number of abortions occurring inside or outside the formal health care system, is the sad reality that abortion is widely sought after and available for women in every U.S. state. There is both a supply and demand issue when it comes to abortion in America. While most abortions are still performed in women’s states of residence, the number of women traveling out of state to obtain an abortion increased by 126% from 2020 to 2023. The data detailed in this paper should make the American people and their elected representatives realize that abortion remains widely available and legal in America – even in states where the media and many government officials want to have the public believe that no abortions are occurring within state lines, or that unfettered abortion should occur between every state’s lines. The data should also make these same constituencies realize that the conversation about post-Dobbs abortion data is complex and has many limitations that are a result of the ongoing de-regulation of abortion that makes it difficult to track. As such, it cannot be simplified easily without losing the important contexts of state regulations, abortion shield laws, and telehealth abortions allowing for advance provision, for example. The current number of abortions occurring in America cannot be explained by one phenomenon but rather by detailed explanations of the intricacies of how and where women are obtaining abortions. The total number of abortions in post-Dobbs America is the result of a multitude of factors:
- An increasing number of women from pro-life states are traveling out of state to obtain abortions and obtaining abortion drugs under shield laws. However, a majority of abortions are still being performed on women in their states of residence where abortion is still legal at some or any point in a woman’s pregnancy.
- An increasing number of abortions are being performed via telehealth, but a majority of abortions are still being performed at brick-and-mortar abortion centers.
- Pro-life state laws do not prevent all abortions from occurring, even within state lines. However, they have been responsible for the elimination of abortions performed at brick-and-mortar centers in certain states.
Ultimately, one abortion performed anywhere is one too many and a tragedy. The fact that well over one million are occurring a year is a national travesty.
Mia Steupert, M.A. serves as Research Associate at the Charlotte Lozier Institute.
[1] “Despite Bans, Number of Abortions in the United States Increased in 2023 | Guttmacher Institute,” March 12, 2024. https://www.guttmacher.org/2024/03/despite-bans-number-abortions-united-states-increased-2023.
[2] “HEALTH AND SAFETY CODE CHAPTER 170A. PERFORMANCE OF ABORTION.” https://statutes.capitol.texas.gov/Docs/HS/htm/HS.170A.htm. Texas had previously enacted a heartbeat law in September 2021 before Dobbs. This law prohibited brick-and-mortar abortions after an unborn child’s heartbeat was detected. However, during the period that the law was in effect (September 1, 2021) until the state’s life at conception law went into effect on July 1, 2022, 26,762 abortions occurred in the state. That number dropped to 86 total abortions from July through December 2022, after the life-at-conception law was enacted. Eighteen of the 86 abortions were performed under the exceptions clauses in Texas’ law.
[3] “2024 Tennessee Code: Title 39 – CRIMINAL OFFENSES (§§ 39-1-101 — 39-17-1812): Chapter 15 – OFFENSES AGAINST THE FAMILY (§§ 39-15-101 — 39-15-514): Part 2 – ABORTION (§§ 39-15-201 — 39-15-219): Section 39-15-213 – [See Note] Criminal Abortion – Affirmative Defense.” https://law.justia.com/codes/tennessee/title-39/chapter-15/part-2/section-39-15-213/.
[4] “SENATE ENROLLED ACT No. 1 (ss).” https://iga.in.gov/pdf-documents/122/2022ss1/senate/bills/SB0001/SB0001.06.ENRH.pdf
[5] Society of Family Planning (2023). “#WeCount Report: April 2022 to December 2022.” https://doi.org/10.46621/143729dhcsyz.
[6] McCann, Allison. “Inside the Online Market for Overseas Abortion Pills.” The New York Times, April 13, 2023, sec. U.S. https://www.nytimes.com/interactive/2023/04/13/us/abortion-pill-order-online-mifepristone.html.
The 2022 data used in the media report was reported by the CDC, the only federal, albeit voluntary, source of reporting on abortion and was woefully incomplete.
[7] Shah, Simmone. “What Abortion Safe Haven States Can Do.” TIME, June 27, 2022. https://time.com/6191581/abortion-safe-haven-states/.
[8] A point of clarification regarding terminology: mail-order abortions are not always performed using a telehealth platform. Only mail-order abortions occurring within the formal health care system utilize telehealth platforms. Mail-order abortions occurring outside of the formal health care system do not use FDA-approved telehealth platforms. When mail-order abortions utilizing telehealth platforms are being referred to in this paper the author will use the terms “mail order, telehealth” or “telehealth” abortions interchangeably. For mail-order abortions occurring outside of the formal health care system, the author will use the term “mail-order abortions” or “self-managed abortions.” Self-managed abortions can also refer to the ingestion of herbs or other non-indicated medications with the sole intent of ending one’s pregnancy. When discussing self-managed abortions, this paper is referring to self-managed abortions carried out via abortion drugs obtained outside of the formal U.S. health care system. These drugs can be provided by international online organizations, online e-commerce websites, and community network support groups.
[9] Post-Dobbs data in the context of this paper refers to the years 2023 and 2024 as the 2022 data provided by SFP’s #WeCount project was not a full year’s worth of data, reflected a legal landscape that has since greatly changed, and represented a time when many laws were in legal limbo.
[10] Varney, Sarah. “Some Red States Report Zero Abortions. Doctors and Researchers Say It’s Not True.” NPR, February 13, 2025, sec. Shots – Health News. https://www.npr.org/sections/shots-health-news/2025/02/13/nx-s1-5293523/abortion-data-states-bans.
[11] “Questions and Answers on Mifepristone for Medical Termination of Pregnancy Through Ten Weeks Gestation.” FDA. https://www.fda.gov/drugs/postmarket-drug-safety-information-patients-and-providers/questions-and-answers-mifepristone-medical-termination-pregnancy-through-ten-weeks-gestation.
[12] American Civil Liberties Union. “FDA REMS Review Announcement Letter.” December 16, 2021. https://www.aclu.org/documents/fda-rems-review-announcement-letter.
[13] The FDA did not issue a written statement announcing this regulatory change. Instead, the agency discreetly updated its website page on mifepristone to reflect the agency’s permanent changes. Relatedly, the agency’s Q and A page for mifepristone was also changed and GenBioPro, an American manufacturer of mifepristone, released a statement detailing the change made by the agency.
[14] #WeCount Report: April 2022 to December 2022.
[15] Society of Family Planning (2024). “#WeCount Public Report: April 2022 to September 2023.” https://doi.org/10.46621/675707thmfmv.
[16] Society of Family Planning (2024). “#WeCount Public Report: April 2022 to June 2024.” https://doi.org/10.46621/728122kflzwf.
[17] McDonnell, C. “Understanding the Mail-order Abortion Rules Within the Federal ‘Comstock Act,’” Americans United for Life. https://aul.org/wp-content/uploads/2024/08/Federal-mail-order-abortion-rules-report.pdf
[18] KFF. “Abortion in the United States Dashboard.” https://www.kff.org/womens-health-policy/dashboard/abortion-in-the-u-s-dashboard/. Those states include Alabama, Arkansas, Idaho, Indiana, Kentucky, Louisiana, Mississippi, Oklahoma, South Dakota, Tennessee, Texas, and West Virginia. Wisconsin had a life-at-conception law in effect until September 2023 when a state court enjoined the law. The law’s injunction made abortion legal in the state through 22 weeks. Similarly, North Dakota was enforcing a life-at-conception law until September 2024 when a state court enjoined the law. Abortion is now legal in North Dakota throughout all nine months because of the broad exceptions to the state’s viability law.
[19] States that prohibit abortion after a fetal heartbeat include Iowa, Florida, Georgia, and South Carolina. States that limit abortion at other pre-viability gestational ages include Nebraska (12 weeks), North Carolina (12 weeks), Ohio (22 weeks of gestation), and Utah (18 weeks). Pennsylvania and New Hampshire limit abortion after 24 weeks.
[20] “State of Telehealth Medication Abortion (TMAB).” RHITES. https://www.rhites.org/maps. These states include Alaska, Arizona, Florida, Georgia, Iowa, Missouri, Nebraska, North Carolina, North Dakota, South Carolina, Utah, and Wisconsin.
[21] KFF. “Abortion in the United States Dashboard.” These states include Arizona, California, Maryland, Michigan, Missouri, Montana, Nevada, New York, and Ohio.
[22] The nine states with post-viability limits that do not in practice substantially protect the unborn include Connecticut, Delaware, Hawaii, Maine, Massachusetts, Rhode Island, Virginia, Washington, and Wyoming.
[23] These states include Alaska, Colorado, Maryland, Michigan, Minnesota, New Jersey, New Mexico, Oregon, and Vermont.
[24] Harned, Mary E. “Abortion ‘Shield Laws’: Pro-Abortion States Seek to Force Abortion on Life-Affirming States.” Charlotte Lozier Institute, August 24, 2023. https://lozierinstitute.org/abortion-shield-laws-pro-abortion-states-seek-to-force-abortion-on-life-affirming-states/.
[25] Cohen, David S., Greer Donley, and Rachel Rebouché. “Abortion Shield Laws.” Edited by C. Corey Hardin. NEJM Evidence 2, no. 4 (March 28, 2023). https://doi.org/10.1056/EVIDra2200280.
[26] The 14 states include Arizona, Connecticut (and Public Act No. 22-19, 2022), Delaware, Hawaii, Illinois, Maryland, Michigan (and Executive Order No. 2022-5), Minnesota, Nevada, New Jersey (and N.J. Stat. §2A:84A-22.19), New Mexico, North Carolina (and Executive Order No. 8, 2025), Oregon, and Pennsylvania. Arizona, Michigan, North Carolina, and Pennsylvania enacted shield laws via executive order while the remaining states and D.C. enacted their respective shield laws via the legislative process.
[27] The eight states include California, Colorado, Maine, Massachusetts, New York, Rhode Island (and S2262 Substitute B, 2024), Vermont, and Washington. For six of these eight states’ shield laws (CO, ME, MA, NY, RI, and VT) the law requires that the shielded abortionist be licensed to perform abortions in the shielding state AND physically reside in the shielding state. California and Washington’s shield laws only specify that the shielded “provider” be licensed to perform abortions in the shielding state.
[28] “#WeCount Public Report: April 2022 to June 2024.” SFP.
[29] These totals were calculated using the Ineedana and Abortion Finder databases. The totals are current as of February 19, 2025, but are subject to change as centers open and close quicker than the databases are updated and because these totals are point-in-time totals that change as state laws change. Not all hospitals/doctors’ offices that perform abortions are included in databases. Therefore, the number of brick-and-mortar centers is an undercount because it is not possible to capture the true total of all the hospitals that perform abortions using publicly available databases. This issue is compounded by the fact that many states do not report abortion totals by facility so abortion-performing hospitals that do not turn up in the databases are not listed in public-facing, state-published reports.
[30] The descriptions and totals contained in Tables 2-7 in Appendix B, as well as Table 8 in Appendix C, were collected using the information on the Plan C website. Plan C is a website for women to find information on where they can order and obtain abortion drugs based on the state in which they reside. Plan C’s information was cross-checked with totals available within the Ineedana and Abortion Finder databases.
[31] Cohen, David S., Greer Donley, and Rachel Rebouché. “Abortion Pills.” Stanford Law Review 76, no. 2 (February 2024): 317–402. https://www.stanfordlawreview.org/print/article/abortion-pills/.
[32] Ibid. Until July 2023, Aid Access operated outside the formal U.S. health care system as an internationally based online organization. This means that the abortionists who were mailing abortion drugs to women in the United States were abortionists licensed in other countries and that the drugs were not coming from an FDA-approved manufacturer. However, in July 2023, Aid Access became “completely US provider-led,” meaning that the drugs were now being dispensed by abortionists licensed in shielding states, the drugs being sent to women were coming from an FDA-approved manufacture, and the organization is now operating within the formal U.S. health care system.
[33] There are a number of region-specific Planned Parenthood affiliates owned and overseen by the larger Planned Parenthood organization listed above. When Planned Parenthood is considered as one entity, there are 20 unduplicated U.S.-based, online-only organizations/centers that provide women in certain states with mail-order abortion drugs via telehealth.
[34] Gleckel , Jareb A., and Sheryl Wulkan. “Abortion and Telemedicine: Looking Beyond COVID-19 and the Shadow Docket.” UC Davis Law Review 54 (May 2021): 105–21. https://lawreview.law.ucdavis.edu/archives/54/online/abortion-and-telemedicine-looking-beyond-covid-19-and-shadow-docket.
[35] As of February 19, 2025, there were three e-commerce sites listed on Plan C’s website. However, the number of organizations and websites listed on Plan C’s website changes frequently, which is why this paper uses a point-in-time total. This paper will use the total of three to remain consistent with the same point-in-time mark of February 19 for databases used to calculate other provider totals. The three websites captured by CLI’s research as of February 19 do not represent the totality of websites that exist, but rather the ones that were documented on Plan C’s website when the original research for this paper was conducted. Plan C does not explain why they add or remove providers from their website.
[36] India leads the world in the number of abortion drug manufacturers (37). China and Vietnam each have three abortion drug manufacturers, the U.S. has two, and Canada, France, Germany, Nepal, Russia, Spain, and Switzerland each are home to one manufacturer.
[37] Kitchener, Caroline. “Covert network provides pills for thousands of abortions in U.S. post Roe.” Washington Post. October 18, 2022. https://www.washingtonpost.com/politics/2022/10/18/illegal-abortion-pill-network/.
[38] To see the breakdown by state, see Table 7 in Appendix B.
[39] Because of the lack of a federal reporting mandate, California, Maryland, New Hampshire, and New Jersey do not report data to the CDC.
[40] Steupert, Mia. “The State of Abortion Reporting in 2024 America: Still Striving Toward a Better National Standard.” Charlotte Lozier Institute, American Reports Series, Issue 26. June 26, 2024. https://lozierinstitute.org/the-state-of-abortion-reporting-in-2024-america-still-striving-toward-a-better-national-standard/. California, Maryland, Michigan, New Hampshire, and New Jersey are not required by their respective state laws to report abortion data. North Dakota’s abortion reporting law is still in effect but when the North Dakota Department of Health and Human Services released the state’s 2022 abortion data, the report noted that the state would no longer be releasing any annual abortion reports. Furthermore, it is important to note that while five states (Hawaii, New Mexico, Rhode Island, Tennessee, and Washington) and Washington D.C. are required to release state-published abortion reports, they have not in years and only have submitted 2022 abortion data to the CDC.
[41] Ibid.
[42] CLI emailed every health department that publishes abortion data either on their department website, upon request, or only to the CDC to see if their state’s published abortion totals included telehealth abortions prescribed by providers in and outside of the state. Because states that have largely prohibited brick-and-mortar abortions are no longer reporting abortion totals in depth or at all (despite telehealth abortions still occurring in their states), CLI only emailed the health departments in states where abortion is still legal at some gestational age. To see which states’ health departments do or do not report telehealth abortion data, see Table 9 in Appendix D.
[43] Jones RK, Kirstein M, Philbin J. Abortion incidence and service availability in the United States, 2020. Perspect Sex Reprod Health. 2022;54(4):128‐141. https://doi.org/10.1363/psrh.12215
[44] “Monthly Abortion Provision Study.” Guttmacher Institute. June 21, 2024. https://www.guttmacher.org/monthly-abortion-provision-study.
[45] The Guttmacher Monthly Abortion Provision totals used in the calculations for this paper were taken from the project’s website and data files on February 19, 2025, and contained data for 2023 – October 2024. On February 27, 2025, the Monthly Abortion Provision Study released November 2024 totals, but those state-level totals were not included in this paper. To find the data utilized by CLI in this paper, download the previously published estimates Excel sheet in the study’s metadata files from the 1-22-2025 data folder.
[46] However, as noted elsewhere in this paper, even in states where brick-and-mortar abortions are illegal many women still obtain abortions by taking advantage of access in other states where abortionists are protected by shield laws.
[47] The most recent #WeCount report was released in October 2024 and was the first to start including abortions provided under shield laws and capture them as occurring in the states where the drugs were mailed. This change makes #WeCount’s data the only publicly available data to include abortions performed under shield laws in states where brick-and-mortar abortions are largely prohibited.
[48] “#WeCount Public Report: April 2022 to June 2024.” SFP.
[49] Both Guttmacher and #WeCount report rounded estimates within a statistical uncertainty level with upper and lower bounds; not exact abortion counts.
[50] “#WeCount Report: April 2022 to June 2024” (Society of Family Planning, October 22, 2024), https://societyfp.org/wp-content/uploads/2024/10/WeCount-Report-8-June-2024-data.pdf.
[51] AE Fiastro et al., “Patient Characteristics Associated with Choosing Telehealth vs. In-Clinic Medication Abortion Care,” Contraception 121 (May 1, 2023): 110019, https://doi.org/10.1016/j.contraception.2023.110019.
[52] #WeCount does not publish data for pre-Dobbs monthly abortions except for April and May 2022 or data from 2020 and 2021 when the FDA’s REMS for abortion drugs initially changed. This is why those totals cannot be included in Figure 3 for a more complete comparison of how different policy changes other than Dobbs are impacting how women are obtaining abortions.
[53] Amy Friedrich-Karnik, Isabel DoCampo, and Candace Gibson, “Medication Abortion Remains Critical to State Abortion Provision as Attacks on Access Persist,” guttmacher, February 25, 2025, https://www.guttmacher.org/2025/02/medication-abortion-remains-critical-state-abortion-provision-attacks-access-persist.
[54] Abigail R. A. Aiken et al., “Provision of Medications for Self-Managed Abortion Before and After the Dobbs v Jackson Women’s Health Organization Decision,” JAMA 331, no. 18 (March 14, 2024): 1558–64, https://doi.org/10.1001/jama.2024.4266.
[55] The data covered in this study’s time period was before Aid Access, the organization highlighted in the study, was considered to be operating within the formal health care system. Therefore, these numbers very likely changed when Aid Access began exclusively utilizing U.S. abortionists when shipping drugs within the United States and started operating within the formal U.S. health care system. For this reason, this data shouldn’t be extrapolated for this type of abortion provision at any time after this study period. Furthermore, the data included in this study was only from states that allowed telemedicine abortions at the time that the study was conducted (March 1 – December 31, 2022). Given the study’s self-reported limitations, the numbers within this table are an undercount and likely not completely representative of the most current estimates but were described to give readers a general sense of historical, post-Dobbs estimates. While Aid Access no longer would be included in the estimates within Table 10, it is not unreasonable to believe that other abortion drug providers operating outside the formal health care system became more popular in Aid Access’ absence. Media reports have confirmed that other informal abortion drug providers were being heavily utilized in addition to Aid Access. For example, Las Libres was the second most popular outlet for women seeking abortion drugs outside the formal health care system when Aid Access occupied the top spot.
[56] This table was created using data from the Aiken et al., March 2024 study.
[57] 2,876 of the 6,919 total abortions for this mode of provision were imputed by the authors from additional online websites that didn’t respond to the authors’ study questions.
[58] No literature existed on the average usage rate of abortion drugs sold by online websites, so the study’s authors used the lowest published usage rate from the four studies found in footnote 38 for telehealth organizations as they believed that online websites were more similar in operation to international telehealth organizations than community networks.
[59] Abigail R. A. Aiken et al., “Requests for Self-Managed Medication Abortion Provided Using Online Telemedicine in 30 US States Before and After the Dobbs v Jackson Women’s Health Organization Decision,” JAMA 328, no. 17 (November 1, 2022): 1768–70, https://doi.org/10.1001/jama.2022.18865.
[60] Allison McCann, “Inside the Online Market for Overseas Abortion Pills,” The New York Times, April 13, 2023, sec. U.S., https://www.nytimes.com/interactive/2023/04/13/us/abortion-pill-order-online-mifepristone.html.
[61] This table was created using data from a New York Times article published in April 2023.
[62] The article didn’t specify the number of pills sent in the drug regimens mailed to women so the total number of women receiving drugs was included instead.
[63] Abigail R. A. Aiken et al., “Advance Provision of Mifepristone and Misoprostol via Online Telemedicine in the US,” JAMA Internal Medicine 184, no. 2 (January 2024): 220–23, https://doi.org/10.1001/jamainternmed.2023.7291.
[64] #WeCount abortion totals were obtained from Tables 1-2023 and 1-2024 in its most recently released report. Guttmacher abortion totals for 2023 – October 2024 were obtained from the metadata associated with the Monthly Abortion Provision Project. The spreadsheet titled “MonthlyAbortionProvisionMonthly” was downloaded and analyzed to calculate the estimated totals reported by Guttmacher from 2023 through October 2024. This data revealed that the total number of abortions in the U.S. in 2023 listed within the spreadsheet (1,032,140) and that appeared on the project’s dashboard was higher than the total number of abortions for 2023 if someone added the total number of abortions in each of the 50 U.S. states and D.C. for that same year (1,029,240). The reason for the discrepancy is not provided by the Guttmacher Institute. Additionally, the discrepancies between #WeCount’s and Guttmacher’s data are not solely because Guttmacher’s data does not include shield law abortions. The methods utilized by the two organizations differ slightly. Guttmacher’s numbers are estimates obtained through survey samples while #WeCount’s data are obtained through surveying all abortion centers and virtual organizations. Not all centers and organizations answered, however, and the exact response rates are not described in either study’s description of its methodology. Lastly, because Guttmacher uploaded new data and slightly revised older monthly estimates after this paper was researched and written but before it was published, the calculations in this paper don’t quite match the most current data on Guttmacher’s project dashboard or most updated metadata Excel sheets but rather reflect previously published estimates.
[65] Elissa Nadworny, “Despite State Bans, Abortions Nationwide Are up, Driven by Telehealth,” NPR, May 14, 2024, https://www.npr.org/sections/health-shots/2024/05/14/1251086997/abortion-increase-research-wecount-telehealth.
[66] “Despite Bans, Number of Abortions in the United States Increased in 2023,” Guttmacher Institute.
[67] “Monthly Abortion Provision Study.” Guttmacher Institute.
[68] This data was obtained from Guttmacher’s metadata associated with the Monthly Abortion Provision project. The spreadsheet titled “MonthlyAbortionProvision_Travel_2020_2023” was downloaded and analyzed to calculate the data on women traveling out of state in 2023 and changes in the data from 2020 to 2023. Guttmacher’s Monthly Abortion Provision study does not have residence data for 2024.
[69] These 21 states include Alaska, Arizona, California, Colorado, Connecticut, Delaware, Hawaii, Maine, Maryland, Massachusetts, Michigan, Montana, Nebraska, New Jersey, Nevada, New York, Oregon, Pennsylvania, Utah, Virginia, and Washington.
[70] These four states include Iowa, New Hampshire, Rhode Island, and Wyoming.
[71] In Vermont, nonresident abortions increased while resident abortions decreased in 2023.
[72] The percentages of nonresident versus resident abortions data in this table and in the previous paragraph were taken from the spreadsheet titled “MonthlyAbortionProvision_Travel_2020_2023” within the Previously Published Estimates, 01_22_2025 folder associated with the project’s metadata. These percentages were applied to the 2020 abortion totals in Guttmacher’s Abortion Provider Census published in 2022 and the 2023 totals within the Monthly Abortion Provision spreadsheet titled “MonthlyAbortion ProvisionMonthly” in the Previously Published Estimates, 01_22_2025 folder.
[73] “Induced Abortion Report, 2023,” Branch of Health Statistics, Arkansas Department of Health. https://healthy.arkansas.gov/wp-content/uploads/Induced_Abortion_2023_vital_stat.pdf.
[74] “Abortion Surveillance in Oklahoma, 2002-2023 Summary Report,” Oklahoma State Department of Health. May 6, 2024. https://oklahoma.gov/content/dam/ok/en/health/health2/aem-documents/data-and-statistics/center-for-health-statistics/induces-termination-of-pregnancy/2023%20AbortionReport.pdf
[75] “South Dakota, 2023 Report of Induced Abortions,” South Dakota Department of Health, Office of Health Statistics. July 2024. https://doh.sd.gov/media/fdth1jyh/2023-abortion-report.pdf
[76] To be clear, no abortion reports released by any state, pro-life or pro-abortion, provide accurate and complete data on the number of telehealth abortions occurring in states or residents traveling out of state to obtain abortions; it is not just pro-life states whose reports are lacking in accuracy and completeness.
[77] “#WeCount Public Report: April 2022 to June 2024.” SFP. Those 10 states include Alabama, Arkansas, Kentucky, Louisiana, Mississippi, Missouri, South Dakota, Tennessee, West Virginia, and Georgia.
[78] These three states include Idaho, Oklahoma, and Texas.
[79] This table was created using data from Figures 9-21 in #WeCount’s latest report. Figure 21 in the #WeCount report is incorrect. The in-state total is 11,985, not 9,065, as noted in the paragraph above the figure.
[80] Jones, Rachel K., Marielle Kirstein, and Jesse Philbin. “Abortion Incidence and Service Availability in the United States, 2020.” Perspectives on Sexual and Reproductive Health 54, no. 4 (December 2022): 128–41. https://doi.org/10.1363/psrh.12215.














