










An Overview of Online Abortion Drug Access in Post-Dobbs America


This is Issue 42 of the American Reports Series.
Executive Summary
- Eight online-only organizations are violating pro-life state laws by shipping abortion drugs into those states.
- Of online abortion drug sellers within the formal U.S. healthcare system that publicly report the gestational age at which they will ship abortion drugs, only 19% complied with the FDA’s requirement to not ship the drugs after 70 days’ gestation. This means 64 sellers violated the FDA’s safety limit.
- Of 28 websites the FDA sent abuse letters to in 2019, 10 are still active and breaking federal law by selling unapproved and misbranded abortion drugs to U.S. women.
- Federal law prohibits the mailing of abortion drugs within the formal U.S. healthcare system and the importation of unapproved abortion drugs outside of the formal healthcare system. However, the federal government hasn’t enforced these laws.
All estimates, calculations, and tables in this paper and the associated appendices are point-in-time estimates current as of March 1, 2026. As such, new online abortion drug providers may have been established since this date, and/or other changes to online abortion drug access and provision may have occurred.
Note: This paper was drafted before May 1, 2026, when the U.S. Court of Appeals for the Fifth Circuit granted Louisiana’s motion to stay the 2023 Risk Evaluation Mitigation Strategy (REMS) for the abortion drug, mifepristone. This ruling meant that abortion drugs could not be sent through the mail, and women had to visit an abortion provider in person before receiving the abortion drug while the outcome of the litigation is pending. On May 4, 2026, the Fifth Circuit’s pause on the 2023 REMS for mifepristone was itself temporarily stayed by the United States Supreme Court. Supreme Court Justice Samuel Alito extended the court’s stay on May 11, 2026, and again on May 14, 2026, while litigation continues in lower courts. As of May 20, 2026, the 2023 REMS remain in effect.
The Appendices for this paper can be found at the following address: https://lozierinstitute.org/wp-content/uploads/2026/05/American-Reports-42-Appendices.pdf
Introduction
In a post-Dobbs America, abortion provision has greatly shifted from when Roe v. Wade was the controlling legal precedent across the country. As of May 2026, 13 states prohibit abortion, with other states like Wisconsin enforcing such a law for a little over a year post-Dobbs and Missouri enforcing a life-at-conception law until a ballot initiative nullified the law in November 2024.[1] Because of the prohibition on abortions in these 13 states, abortions are increasingly being obtained in subversion of state law via telehealth from physicians operating in other states.[2] In four states, abortions are prohibited after a fetal heartbeat, and in two states, abortions are prohibited after 12 weeks.[3] In three of the states with gestational limits on abortion, explicit telehealth abortion limits or prohibitions exist as well.[4]
To be clear, a majority of abortions in America are still being performed in person at brick-and-mortar abortion facilities in states where such abortions are still legal. In 2024, the last full year of data reported by SFP’s #WeCount project, around 78% of the country’s total abortions were performed in person at brick-and-mortar facilities while around 22% were performed via telehealth. However, while the discrepancy between the two modalities is still significant, it is important to consider that from April through June 2022, roughly 5% of all U.S. abortions performed within the formal healthcare system were via telehealth. That percentage increased to 20% from April through June 2024 and 27% from April through June 2025.[5]
Several factors and legal changes are responsible for the shifts in the supply and ensuing demand for abortion, besides the Dobbs decision. Changes to mifepristone’s Risk Evaluation and Mitigation Strategies (REMS) requirements by the United States Food and Drug Administration (FDA), a subsequent increase in the proliferation of foreign and domestic online providers of abortion drugs, and the enactment of shield laws all contributed to a post-Dobbs landscape where abortion drugs are readily available on all corners of the internet to women in all 50 states and D.C.[6]
Part one of this paper will serve as an overview of the state of online abortion provision and access in America and the available online providers in and outside of the United States. The paper will first touch on the basics of abortion drugs, telemedicine, telehealth, and the legal landscape surrounding online access to abortion drugs.[7] Part two will go into detail about each category of online abortion drug provider and which providers, if any, follow the FDA’s REMS requirements.[8]
Part 1
The Basics of the Abortion Drug Regimen
Online abortion access strictly utilizes abortion drugs. In the United States, drug-induced abortions (both in-person and via telehealth) are the most common type of abortion, with 63% of the total number of abortions in 2023 being drug-induced. Regardless of how women obtain abortion drugs, the most widely available and used method is a two-drug regimen involving mifepristone and misoprostol. The first drug, mifepristone (in the form of one 200-milligram pill), is taken orally to block progesterone, a hormone needed to sustain pregnancy. Twenty-four to 48 hours later, the woman takes four 200-milligram misoprostol pills vaginally or buccally to induce contractions to expel the dead unborn baby and associated pregnancy tissue.
Mifepristone, originally known as RU-486, was first developed in the 1980s by French researchers to be taken alongside misoprostol to induce an abortion. While the U.S. initially prohibited the importation of Mifepristone, the FDA approved it for market use in September 2000. Danco was licensed as the drug’s sponsor and manufacturer and distributed the drug in the U.S. under the brand name Mifeprex. Danco’s headquarters are in New York, but Mifeprex is manufactured in Spain. GenBioPro manufactures a generic version of mifepristone approved by the FDA in 2019. GenBioPro’s headquarters are in Las Vegas, Nevada, but their version of mifepristone is manufactured in India. Lastly, another generic version of the drug, manufactured by Evita Solutions, was approved by the FDA on September 30, 2025.[9] Other FDA-approved uses for mifepristone include the management and treatment of hyperglycemia stemming from Cushing Syndrome, albeit at a different dosage than that used for abortion. Researchers have also promoted the off-label use of mifepristone for emergency contraception and the treatment of uterine fibroids.
Misoprostol was discovered and developed in 1973 at Searle and first approved by the FDA in 1988 for the prevention and treatment of gastric ulcers caused by NSAIDs. The FDA approved it under the brand name Cytotec, which was manufactured, sponsored, and distributed by Pfizer. When the FDA approved mifepristone in 2000, misoprostol was approved in conjunction with mifepristone to form the popular abortion drug regimen. Over the years, the FDA has approved generic versions of misoprostol manufactured and sponsored by ANI Pharms, ACQ Pharma, and Micro Labs. Off-label uses for misoprostol include second-trimester abortions (as a single drug or in conjunction with methotrexate) as well as other uses such as the management of miscarriages.
For abortion, the FDA has only approved the abortion drug regimen of mifepristone and misoprostol. It has never approved the use of misoprostol alone for abortion. However, misoprostol is prescribed off-label for misoprostol-alone abortions. While the American College of Obstetricians and Gynecologists (ACOG), as well as Planned Parenthood, promote misoprostol-alone abortions in the instance that mifepristone is unavailable, this regimen is rarely used in the United States.
The Basics of Telemedicine
Telemedicine is a way to expand access to healthcare for those who live far from traditional brick-and-mortar facilities by utilizing technology. When considering the topic of online healthcare in general, it is important to differentiate between telemedicine, telehealth, and telecare (sometimes referred to as “mHealth”). “Telemedicine” refers to the use of technology to deliver diagnostic, medical, and treatment (clinical) services. An example of a telemedicine service would be monitoring a patient’s recovery after surgery. There are three main modalities used in modern-day telemedicine: synchronous, asynchronous, and remote patient monitoring. Synchronous models of telemedicine utilize live, two-way, real-time audio or visual feeds between patients and providers. Synchronous video models are the ones most covered by insurance providers and Medicaid/Medicare because they allow for a doctor-patient relationship similar to in-person care. By contrast, asynchronous models, otherwise known as store-and-forward models, allow patients and providers to exchange medical information (such as imaging and lab results) through non-real-time communications on messaging platforms.
“Telehealth,” as a colloquial term, evolved from the term “telemedicine.” Telehealth involves a broader range of services, often non-clinical, provided by more than just doctors. With telehealth, nurses, pharmacists, etc., can render educational services and provide social support services. Organizations that provide abortion drugs via telehealth often utilize the same modalities as telemedicine (synchronous, asynchronous, and remote patient monitoring) but differ from telemedicine in that non-clinical services are rendered.[10] Furthermore, the provision of telehealth abortions differs from the provision of telemedicine abortions in that regulations and standards of care surrounding telemedicine and even other forms of telehealth define care as occurring where the patient is located. When telehealth abortions are provided via shield laws and virtual-only organizations and mailed into pro-life states, however, the abortion industry and proponents of shield laws consider the abortion to have occurred in the shielding state. Lastly, telemedicine standards of care, as well as state laws, require that telemedicine providers be licensed in the state where the patient is located. This does not occur when abortionists mail abortion drugs to women in pro-life states. The abortion providers are typically only licensed in the shielding states.[11]
“Telecare” is used interchangeably with the term “mHealth.” These modalities specifically involve informal consumer-based services like fitness apps, electronic sensors on phones or watches, and other mobile devices that operate outside of any provider interaction. These modalities do not involve obtaining abortion drugs online from sources either within or outside of the formal American healthcare system.
The Basics of Telehealth Abortion and Ordering Abortion Drugs from Other Online Sources
U.S.-based online-only organizations and hybrid brick-and-mortar facilities that mail abortion drugs operate within the formal American healthcare system. These means of obtaining drug-induced abortion count as “telehealth” in the context of the existing research framework used to describe the online provision of abortion drugs. Such organizations are considered to operate within the formal healthcare system because they involve U.S.-licensed healthcare professionals, and the drugs they provide have been produced within the FDA-approved supply chain. On the other hand, abortion drugs that are sent via international online organizations, e-commerce pharmacies, and community networks don’t operate within the formal American healthcare system and often don’t utilize any healthcare providers. These entities are considered to operate outside of the formal healthcare system because they don’t utilize U.S.-licensed healthcare professionals, and they ship abortion drugs produced outside of the FDA’s approved supply chain.[12] Abortion drugs obtained via formal American telehealth organizations and those obtained separately from other informal online sources will both be covered in this paper.
Below, the different types of online abortion providers are defined in-depth:
1. Telehealth abortion providers that operate within the formal U.S. healthcare system and mail abortion drugs to women around the country
-
- Virtual-only organizations
-
-
- Virtual-only organizations use telehealth platforms to prescribe and mail U.S. women abortion drugs. With these organizations, the general process is as follows: the associated abortionists review a prospective patient’s electronically submitted medical intake form. Depending on the organization, sometimes the abortionist will be required to consult with the woman asynchronously or synchronously to discuss the woman’s eligibility for a mail-order abortion. If the woman is deemed eligible to take the abortion drugs, she and the abortionist will complete the necessary REMS-mandated forms, and the provider will send a prescription for the abortion drug regimen to a REMS-certified pharmacy, such as Honeybee Health, which then mails the drugs to the woman. Some organizations require women to follow up with them after they take mifepristone and misoprostol, while others don’t. There are two types of virtual-only organizations: those that utilize shield laws to ship abortion drugs into pro-life states and those that only ship abortion drugs into/within states where abortion and/or telemedicine is still legal. There are eight of the former organizations currently operating and 34 of the latter.[13] Some virtual-only organizations will mail abortion drugs to women who are not currently pregnant so they can keep them on hand to deal with a future pregnancy or provide them to someone else who can’t easily access abortion drugs.
-
-
- Hybrid brick-and-mortar centers
-
-
- These centers, of which there are currently 38, have physical buildings where drug-induced and/or surgical abortions are performed, but they also offer telehealth abortion services.[14] They typically only send abortion drugs within the state where their center(s) are located. However, it is becoming increasingly popular for these centers to send abortion drugs into other pro-abortion states.[15] Telehealth abortions performed by these hybrid facilities follow virtually the same protocol as the U.S. virtual-only organizations and also use either asynchronous or synchronous platforms, depending on the center. Similar to some virtual-only organizations, some hybrid brick-and-mortar centers will mail abortion drugs to women who are not currently pregnant so they can keep them on hand for future pregnancies or provide them to someone who can’t easily access abortion drugs. Hybrid brick-and-mortar centers can either dispense abortion drugs via the mail from their own centers/certified prescribers or through mail-order, REMS-certified pharmacies. Some organizations require women to follow up with them after they take mifepristone and misoprostol, while others don’t.
-
2. Online abortion drug providers/sources that operate outside of the formal U.S. healthcare system and mail abortion drugs to women around the country
-
- International, online organizations
- The three international online organizations that provide U.S. women with abortion drugs (Telefem Mexico, Abortion Pills in Private, and Women on Web) employ medical professionals licensed in foreign countries, are based in foreign countries, and provide non-FDA-approved drugs manufactured outside of the FDA’s approved supply chain.[16] These organizations don’t require women to meet with the abortionists synchronously or asynchronously before the drugs are sent to them. The woman’s online intake form is the only step she must complete besides payment and signing consent forms (if the organization requires it). All three organizations claim to have a medical professional review the intake forms for eligibility. If a woman is eligible, the organizations send women the abortion drugs from foreign pharmacies or other sources. Because these international online organizations utilize foreign medical professionals, the only support they offer women during or after a drug-induced abortion is providing women with links to or the phone numbers for outside hotlines and support organizations such as the Miscarriage and Abortion Support Hotline.[17]
- International, online organizations
-
- E-commerce websites
- These are typically foreign websites that allow anyone to buy abortion drugs, oftentimes as quickly as an Amazon transaction. These e-commerce websites obtain abortion drugs from international manufacturers and then either ship the drugs directly to the customer or to a U.S. middleman who mails them around the country. The exact location from which these websites operate is often unknown, and the drugs they sell are non-FDA-approved and manufactured outside the FDA’s approved supply chain (despite the websites claiming differently).[18] The headquarters of the drugs’ distributors and manufacturers often differ in location, and both often differ from the location of the drugs’ manufacturing plants.[19] There is absolutely no medical supervision required by these websites, and anyone can buy drugs from most of these websites and have them sent anywhere in the U.S.[20] There are currently eight e-commerce websites vetted by and listed on Plan C’s website, and 10 that CLI discovered when reviewing Sen. Bill Cassidy’s letter to the FDA and through additional research.[21]
- E-commerce websites
-
- Community networks
- These loosely organized groups are composed of community-based distributors who supply U.S. women with free abortion drugs. These networks rely on suppliers who obtain privately donated drugs or drugs from international pharmacies at a low price. Volunteers with these networks distribute the drugs to women via arranged pick-ups or via the mail. Community networks don’t require women to have a prescription when they email the network requesting abortion drugs, nor do any of the five existing community networks offer physician support if women experience post-abortive complications or have questions during or after the drug-induced abortion.[22] The organization Red State Access controls four sub-networks (AccessMA, IdahoAccess, MidwestAccess, and ArkansasTogether), while the network DASH operates independently.[23] Community networks focus on providing their services to women in states with total abortion prohibitions or limits at six or 12 weeks.
- Community networks
To see the categorization of the different types of online abortion providers, see the graphic below:
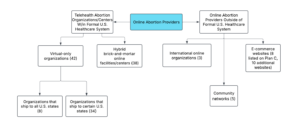
*This graphic was designed by the author using the Lucidspark software.
History of Telehealth Abortion Models
Initially, telehealth abortions in America took place using a site-to-site model where a patient was located in one Planned Parenthood “health” center and an abortionist was located in another “health” center. The patient and abortionist would interact remotely to discuss the logistics and risks of a drug-induced abortion, but the patient received ultrasounds and other pre-abortion screening tests in person, and the drugs were dispensed in person. This model was first introduced in Iowa in 2008 by the Planned Parenthood of the Heartland affiliate and expanded to other Planned Parenthood affiliates in Alaska, Hawaii, Maryland, Montana, Nevada, and New York. Gynuity Health Projects received a special approval from the FDA to test a new telehealth abortion model, the direct-to-patient model, from 2016 to 2021, when it was conducting its TelAbortion Study.[24] This model involved patients receiving in-person, pre-abortion screenings such as ultrasounds, but receiving pre-abortion counseling via telehealth and abortion drugs via the mail. This model evolved during the COVID-19 pandemic as a result of the 2021/2023 REMS modifications and other legal changes, ultimately morphing into the direct-to-patient “no-test” model. This model omitted pre-abortion, in-person screenings and ultrasounds altogether, and continued remote consultation and dispensing of abortion drugs via the mail. This is the model used today by virtual-only organizations as well as almost all hybrid brick-and-mortar facilities.[25]
The Telehealth Abortion and Online Abortion Legal Landscape
This section provides an overview of the regulations that make telehealth abortions available inside the formal U.S. healthcare system, as well as the federal statutes that should be prohibiting the domestic and international shipping of abortion drugs. Ongoing litigation surrounding telehealth abortion is also covered.
Mifepristone’s Risk Evaluation and Mitigation Strategy (REMS)
The regulatory structure that allows abortion drugs to be legal, available, and accessible via telehealth is the current U.S. FDA REMS requirements. A Risk Evaluation and Mitigation Strategy (REMS) is an FDA-required drug safety protocol for medications deemed to have serious safety concerns. REMS control the conditions under which certain drugs can be sold and dispensed. Each drug’s strategy requires specific protocols to ensure the drug is safe to use, such as requiring providers to become certified before prescribing it and/or requiring patients and providers to read the drug’s medication guide before the drug is provided.[26]
REMS requirements were added for Mifeprex in 2011, 11 years after the drug’s initial approval by the FDA in 2000.[27] When the drug was initially approved, it was approved for drug-induced abortions up to seven weeks of gestation (49 days) and had a requirement that mandated in-person administration of the drug. Furthermore, the REMS instituted in 2011 required that Mifeprex only be administered in a hospital or clinic.[28] The REMS for Mifeprex were modified in 2016 to allow for its prescribing until 10 weeks of gestation (70 days). These changes also decreased the number of required in-person visits women had to attend to obtain abortion drugs. In July 2020, a federal district court ruled that the FDA must temporarily suspend enforcement of the in-person REMS requirement for mifepristone due to the COVID-19 pandemic. This ruling allowed for telehealth abortion to be widely utilized for the first time in the United States, in addition to those performed as part of research studies exempted by the FDA, and opened the legal pathway for telehealth abortion to remain legal and available until January 12, 2021. In April 2021, the Biden administration announced the FDA’s decision to waive the in-person requirement for the remainder of the COVID-19 pandemic. The administration formally announced the removal of the in-person requirement in December 2021 and added a requirement that pharmacies that dispense the drug be certified.[29] The removal of the in-person requirement facilitated the rapid proliferation of available virtual-only organizations and hybrid brick-and-mortar centers because it meant that no pre-abortion ultrasound would have to be performed in person. Furthermore, the screenings previously required before abortion drugs were dispensed to a woman, for things like her Rh status and ectopic pregnancies, also did not need to be performed in person. As a 2021 FDA letter claimed, these screenings for gestational age, Rh status, and ectopic pregnancies could be performed safely, virtually, in the FDA’s opinion.
The 2021 REMS modifications were formally approved by the FDA on January 3, 2023, after reviewing Danco’s and GenBioPro’s proposals to comply with the new REMS modifications. While the Alliance for Hippocratic Medicine v. FDA case caused short-lived changes to mifepristone’s REMS program, as of April 2026, the drug is authorized for drug-induced abortions through 70 days of gestation, and the 2023 REMS for mifepristone stands.[30] The REMS involve the following requirements:
1. Mifepristone must be prescribed by a “healthcare” provider certified under the drug’s REMS program, through one of the drug’s three sponsors, and dispensed by a certified provider or certified pharmacy. To become a certified provider, one must complete a prescriber agreement form, which certifies that the provider can:
-
- Accurately assess the duration of a woman’s pregnancy
- Diagnose ectopic pregnancies
- Provide surgical interventions as needed or have the ability to arrange care for women suffering complications, as well as ensure the woman has access to life-saving medical care
- Has read and understands the Prescribing Information from Danco
- Has read the medication guide from Danco’s (or GenBioPro’s or Evita Solutions’) website
- The medication guide outlines the risks and complications associated with taking Mifeprex and educates women on when to contact a healthcare provider if they are suffering post-abortive complications. The guide also lists contraindications to taking Mifeprex and important topics to talk with a healthcare provider about before taking the abortion drugs. Lastly, the guide stresses the importance of follow-up visits to confirm the completion of the abortion, stating, “This follow-up assessment is very important. You must follow-up with your healthcare provider about 7 to 14 days after you have taken Mifeprex to be sure you are well and that you have had bleeding and the pregnancy has passed from your uterus.”
2. The patient agreement form must be reviewed by the patient, signed by the patient and provider, and the woman provided with the medication guide. The patient agreement form confirms:
-
- That the provider has counseled the patient on the risks of Mifeprex included in the Medication Guide provided to the patient, and understands when to seek medical attention if the woman is experiencing post-abortive complications.
- The patient understands what complications to look for, when to contact the provider, and that she should follow up seven to 14 days after she takes mifepristone.
3. Providers must report any deaths from Mifeprex to Danco (or GenBioPro or Evita Solutions for deaths associated with mifepristone in its generic form).
4. Mifeprex may only be dispensed by or under the supervision of a certified pharmacy (one that has completed a pharmacy agreement form, amongst other requirements) that can ship drugs using a shipping service that provides tracking information. The pharmacy agreement form requires that the dispensing pharmacies deliver Mifeprex to the woman within four days of the date the pharmacy received the prescription, except in cases approved by the certified prescriber.
Interestingly, in opposition to informal sources of online abortion drug provision, on the FDA’s webpage for the abortion drug’s REMS, it says:
The FDA does not recommend purchasing mifepristone outside of the Mifepristone REMS program—e.g. buying it online or personally transporting it from a foreign country. If a person does so, they would be bypassing important safeguards specifically designed to protect their health. Prescription medicines that are approved for use in the United States have been reviewed for safety, effectiveness, and quality by the FDA, and are subject to FDA-regulated manufacturing controls, including inspection of manufacturing facilities. Generally, prescription medicines purchased from foreign sources are not the FDA-approved versions. The FDA does not have regulatory oversight of prescription medicines from outside the legitimate U.S. drug supply chain; therefore, the FDA cannot ensure the safety, effectiveness, or quality of those medications.
International and Domestic Laws Governing the Mailing of Abortifacients
Several U.S. laws govern aspects of telehealth abortion and obtaining abortion drugs online from sources operating outside of the formal healthcare system. Thus far, this paper has discussed the REMS requirements that govern the domestic mailing and provision of abortion drugs via telehealth. Under federal law, it is illegal for international organizations, e-commerce websites, and community networks to import abortion drugs into the United States without FDA approval. Federal law (21 U.S.C. § §331(a), 331(d), 355(a)) prohibits the importation into the U.S. and distribution in interstate commerce of misbranded and unapproved drugs. Furthermore, because these abortion drugs are unapproved they also cannot comply with FDA’s REMS requirements. However, these laws are routinely violated by sellers that ship into the U.S. and distribute unapproved and misbranded drugs, with some advertising the abortion drugs on their websites as FDA-approved.[31]
The FDA’s website says on this topic,
In most circumstances, it is illegal for individuals to import drugs or devices into the U.S. for personal use because these products purchased from other countries often have not been approved by the FDA for use and sale in the U.S. If a drug is approved for use in another country but is an unapproved new drug in the U.S. it is illegal to import. The FDA cannot ensure the safety and effectiveness of medicine purchased over the Internet from foreign sources, storefront businesses that offer to buy foreign medicine for you, or during trips outside the U.S. For these reasons, the FDA recommends only obtaining medicines from legal sources in the U.S.
Under the Federal Food, Drug, and Cosmetic Act (FFDCA) (Section 801(d)(1)(B)), it is illegal to import foreign-made versions of FDA-approved drugs that have not been evaluated through the FDA process and prescribers that do not comply with mifepristone’s REMS subsequently violate the FFDCA. The only two exemptions under this law are for drugs authorized by the Secretary of Health and Human Services (HHS) pursuant to a drug shortage, and drugs manufactured outside of the U.S. that have been authorized to be marketed in the U.S. and labeled in accordance with FFDCA requirements. Abortion drugs shipped into the U.S. do not fall under either of those exemptions. The FDA does allow certain exceptions to the prohibition on the importation of foreign drugs under a different regulatory pathway from the FFDCA. The personal importation of foreign drugs is usually allowed for personal use if the drugs aren’t considered risky, the buyer isn’t selling them to others, or the drug is for a serious health condition and unavailable in the U.S. However, it would be hard for the FDA or Customs and Border Patrol (CBP) to argue that abortion drugs are not risky when the FDA placed a black-box warning on Mifeprex and its generic versions because of its safety concerns with the drug(s) and the fact that mifepristone has associated REMS requirements. CBP, the primary agency responsible for administering and enforcing the nation’s drug importation and exportation laws, works with the FDA to determine when these exemptions can be applied. Currently, neither the FDA nor CBP has publicly announced that the importation of foreign abortion drugs meets any of the aforementioned exceptions.
On the domestic front, the Comstock Act prohibits the mailing of abortion drugs within the United States, despite the FDA’s removal of the in-person requirement that initiated the mailing of abortion drugs around the country. An existing provision in the Comstock Act (18 U.S.C. §1461), the original version of which was passed in 1873 and last amended in 1994, prohibits the mailing or shipping of abortifacients through the USPS or express companies, common carriers, or interactive computer services. In theory and by the letter of the law, this should prohibit both virtual-only and hybrid brick-and-mortar facilities, as well as any community networks, from shipping abortion drugs within the United States. In December 2022, the Biden administration’s Office of Legal Counsel (OLC) released a memorandum claiming that statutes 18 U.S.C. §§1461-1462 only apply to the prohibition of mailing abortion drugs for the purpose of performing an unlawful abortion. However, as one legal scholar noted, neither statute contains the word “unlawful,” and the OLC memo’s use of the word comes from case law that doesn’t take the legal history of abortion criminalization in America into consideration (McDonnell, 2025, p. 124-125). Furthermore, McDonnell observes that states (via shield laws, discussed hereafter) do not have the power to nullify a federal law that Congress can and should exercise under its Postal Clause authority (McDonnell, p. 125). Statutes 1461-1462 are still on the books and remain enforceable.
Another provision of the Comstock Act (18 U.S.C. §1462), the original version of which was passed in 1897 and last amended in 1996, prohibits the importation of obscene materials or abortifacients into the United States through an express company or other common carrier or interactive computer service.
Shield Laws
As previously mentioned, after the Dobbs decision, several states had existing life-at-conception laws that went into effect, and several other states passed laws prohibiting abortion at differing gestational ages. Furthermore, some states had or passed legislation explicitly prohibiting the provision of telehealth abortion within the state. To circumvent these different laws, 14 pro-abortion states and D.C. passed laws or executive orders protecting abortionists who provide abortions to patients from pro-life states who traveled to the abortionist’s state to obtain an abortion.[32] Another eight states enacted shield laws that allowed abortionists licensed in their states to ship abortion drugs into states with gestational limits or prohibitions on abortion.[33] Under these shield laws, women can receive the drugs in the mail in a pro-life state from an abortionist associated with one of the eight virtual-only organizations that utilize shield laws in another state. The abortionist who sends these drugs is shielded from prosecution by his state, but is breaking the law of the state where the woman resides. Shield laws have effectively nullified the post-Dobbs pro-life laws in several states. In 2024, shield laws allowed for 76,310 abortion drug regimens to be sent to women in states with full nine-month protections, 25,180 into states with 6-week limits, and 19,340 to women in states with telehealth restrictions.[34]
Ongoing and Closed Federal and State Litigation Regarding Telehealth Abortions[35]
There are currently three ongoing federal court cases involving states suing the FDA. One case, Florida et al. v. U.S. Food and Drug Administration (2025), involves Florida and Texas suing the FDA over its original 2000 approval of mifepristone; the agency’s 2016, 2021, and 2023 REMS modifications; and the agency’s 2019 and 2025 approvals of GenBioPro’s and Evita Solutions’ generic versions of mifepristone. Texas and Florida cited the Comstock Act (18 U.S.C. §1461and 18 U.S.C. §1462) as prohibiting the agency’s 2021/2023 decisions to remove the in-person dispensing requirement and the subsequent availability of telehealth abortions. On April 24, 2026, both Texas and Florida agreed to a stay of the case while the FDA conducts its safety review of mifepristone.
Another case, Louisiana et al. v. U.S. Food and Drug Administration (2025), involves the state of Louisiana and its resident, Rosalie Markezich, suing the FDA over their decision to remove the in-person dispensing requirement in 2021/2023. The plaintiffs argue that the agency’s decisions violated the Administrative Procedure Act (APA) and the Comstock Act. Furthermore, the plaintiffs argue that the removal of the in-person dispensing requirement also caused Markezich to be coerced into getting an abortion because her former partner was able to obtain abortion drugs via telehealth using her name. Those drugs were prescribed by a doctor in California under California’s shield law. The complaint noted that had Markezich been required to attend an in-person consultation prior to her partner receiving the abortion drugs, she could have told a healthcare professional that she wanted the baby, not an abortion. On December 17, 2025, the plaintiffs requested a preliminary injunction of the 2023 REMS modifications and a reinstatement of the in-person dispensing requirements. On April 7, 2026, a Louisiana district court judge sided with the Trump administration’s request to pause the case while the FDA continues its review of the safety of mifepristone, but did note that the plaintiffs had standing and would likely succeed on the merits of the case.[36]
Lastly, in the case of Missouri et al. v. FDA (2024), Missouri, Kansas, and Idaho filed an amended complaint in an attempt to revive the AHM v. FDA case. The amended complaint argued for the reinstatement of the in-person dispensing requirement, amongst other things, and is still active in a Missouri district court.
In addition to these lawsuits against the FDA, pro-life states have sued individual doctors as well as the telehealth organizations the doctors are associated with for utilizing shield laws to ship abortion drugs into pro-life states. In early 2025, Louisiana tried to extradite a New York abortionist, Dr. Margaret Carpenter, after a Louisiana grand jury indicted Carpenter for “criminal abortion by means of abortion-inducing drugs.” In April 2024, Carpenter allegedly sent abortion drugs to a Louisiana woman via telehealth, utilizing New York’s shield law. The woman then used the abortion drugs to coerce her minor daughter to get an abortion that killed the daughter’s unborn child and landed the minor in the hospital. New York Governor Kathy Hochul refused to honor the extradition request. The case, Louisiana v. Carpenter, remains ongoing.
Similarly, in January of 2026, Louisiana tried to extradite California doctor Remy Coeytaux, associated with the online-only organization Aid Access, for allegedly mailing abortion drugs to a Louisiana resident under California’s shield law in 2023. Like Hochul, California Governor Gavin Newsom refused to honor the extradition request, and the case remains ongoing. In Texas v. Aid Access et al. (2026), Texas sued Remy Coeytaux, Aid Access, and Aid Access’s founder, Rebecca Gomperts, for allegedly mailing abortion drugs into the state via telehealth. Texas requested a temporary injunction of all defendants from shipping abortion drugs into the state. Texas also sued a Delaware abortionist, Deborah Lynch, as well as her telehealth abortion organization, Her Safe Harbor, in Texas v. Lynch et al. (2026). The lawsuit requested that Lynch stop mailing abortion drugs into the state. Both Texas cases are pending in Texas state district courts.
To date, there is one ongoing case involving an individual suing a telehealth abortionist (Remy Coeytaux) for shipping abortion drugs that resulted in the wrongful death of an unborn child. In Rodriguez v. Coeytaux (2025), a Texas man, Jerry Rodriguez, sued Coeytaux for mailing abortion drugs via telehealth to Rodriguez’s girlfriend’s estranged husband in violation of Texas’ abortion and wrongful death laws as well as the federal Comstock Act. Rodriguez’s girlfriend’s (Kendal Garza) estranged husband, Adam Garza, who she had not yet divorced but had been living apart from for many years, ordered the abortion drugs that Kendal Garza ended up taking. This is a federal civil case pending in a federal district court in Texas.
In December 2025, South Dakota Attorney General Marty Jackley sent a cease-and-desist letter to Mayday Health, a nonprofit organization organized under the laws of Delaware and headquartered in New York. The attorney general issued the cease-and-desist letter for advertisements Mayday had placed at South Dakota gas stations, directing people to their website, where consumers are further directed to online abortion drug providers such as Abuzz and Aid Access. The order demanded that Mayday Health stop advertising the delivery of abortion drugs via telehealth into South Dakota using pro-abortion shield laws. In a December 19, 2025, letter, Mayday Health refused to stop advertising in South Dakota on First Amendment grounds. In response, the South Dakota Attorney General filed a motion for a preliminary injunction on December 22, 2025, and Mayday Health responded by filing for injunctive and declaratory relief in a New York district court in January 2026. Mayday Health’s request was denied by a federal court solely on procedural grounds. The judge ruled that a state court was the proper venue for the case. A South Dakota circuit court agreed with this and set a trial date for July 2026. However, a settlement was reached, and Mayday Health agreed to remove the gas station advertisements and not place any additional advertisements in South Dakota.
Ongoing State Litigation Regarding Abortion Drugs Provided Outside of the Formal U.S. Healthcare System
In January 2026, North Dakota Attorney General Drew Wrigley issued a cease-and-desist order against Prairie Abortion Fund (PAF), a North Dakota nonprofit, for “promoting and facilitating the unlawful sale of abortion pills in North Dakota.” The order alleged that PAF’s website violated state law by (among other things):
- “Promoting and facilitating the unlawful sale of counterfeit, unapproved, untested, misbranded, or mispresented products”
- “Facilitating and assisting the unlawful sale of products without a required prescription”
- “Promoting, facilitating, and assisting in the unlawful online sale of products that may not be administered without the supervision of a physician”
At the time, PAF’s website linked to other websites that sell abortion drugs. The cease-and-desist order specifically noted that PAF’s website linked to Plan C, which “offers ‘Abortion pills by mail in every state.’” Plan C lists organizations and websites that operate in and outside of the formal U.S. healthcare system. E-commerce websites ybycmeds and Pill Pulse were two examples cited in the North Dakota cease-and-desist order. The order was a result of the Attorney General’s Bureau of Criminal Investigation (BCI) buying abortion drugs from these two websites, without a prescription, without providing any health information, or any form of identification or age verification. The order demanded that PAF stop promoting, linking, or referring individuals to Plan C and the websites contained within Plan C’s website.
Part 2
General Overview of Each Known Website that Provides American Women with Abortion Drugs
How U.S. online-only organizations, international online organizations, hybrid brick-and-mortar centers, e-commerce websites, and community networks operate will now be addressed.
For each organization, center, website, and community network that CLI identified via Plan C’s website, including both those inside and outside of the formal U.S. healthcare system, CLI did an in-depth review of their corresponding website to learn about how the organizations/websites operate, what limitations they place on ordering abortion drugs online (if any), and other information associated with each website (see footnote 13). For the in-depth findings, see Appendix C, Tables 1-5 for each type of online abortion drug provider. Below, the findings of this review are summarized and discussed for each type of online abortion drug provider:
Findings – Telehealth abortion-drug providers that operate within the formal U.S. healthcare system and mail abortion drugs to women around the country
1. Virtual-only organizations (42 total)
- Eight organizations utilize shield laws, and 34 do not.
- Seven of the 41 organizations that publicly report the gestational age at which they will stop shipping abortion drugs to women complied with the REMS requirement that abortion drugs not be prescribed and dispensed after 70 days of gestation. Sixteen organizations stop prescribing/shipping abortion drugs after 77 days, seven after 84, eight after 91, and two after 98 days. One organization claimed to stop prescribing/shipping abortion drugs after the first trimester, and one organization didn’t publicly release this information.[37]
- Nine of the 31 organizations that publicly report whether they require a woman to be of a specific age before sending her the drugs said there was no age requirement for their organization to send women abortion drugs. It depended on the states’ laws regarding minors getting abortions for three organizations. One organization required girls to be 12 or older, one required them to be 15 or older, eight required them to be 16 or older, and one required them to be 17 or older. Eight of the organizations required women to be of legal age (18) or older to obtain abortion drugs from their organizations. Eleven organizations did not publish this information.[38]
- Of the 38 organizations that publicly report whether their organization requires women to participate in a pre-abortion, synchronous video visit to discuss their eligibility for taking the abortion drugs, risks of taking the drugs, etc., 22 organizations required such a video call to take place. Four did not require a video call, and 12 did not require a video call but made the option available for women who had questions they wanted to ask a provider associated with the organization. Four organizations did not report this information.
- Of the 33 organizations that publicly reported whether they sent a telephone number for medical support to the women who were being sent abortion drugs, 30 did provide a number, and three did not. Nine didn’t publicly report this information.
- Seventeen of the organizations allowed for the advanced provision of abortion drugs to women who were not pregnant at the time they requested the drugs, while 24 did not. One organization did not report whether they did or did not.
- Of the nine organizations that reported whether they required a woman to provide a form of identification when she was requesting the abortion drugs, five required an ID, three did not, and one organization required it for women living in certain states. Thirty-three organizations did not publicly report this information.[39]
- For the step-by-step process of ordering abortion drugs, as well as the questions that the public-facing intake forms asked (if any), see Appendix C, Table 1.[40]
- Nine of the 42 virtual-only organizations do not require a woman to follow up virtually seven to 14 days after completing the abortion-drug regimen to ensure a complete abortion. Six organizations require a virtual follow-up, while 27 organizations do not disclose this information on their website.
2. Hybrid brick-and-mortar centers (38 total)
- None of these organizations utilize shield laws to ship abortion drugs to women residing in pro-life states.
- Eight of the 38 organizations that publicly report the gestational age at which they will stop shipping abortion drugs to women complied with the REMS requirement that abortion drugs not be prescribed and dispensed after 70 days of gestation. Twenty-one organizations stop prescribing/shipping abortion drugs after 77 days, and seven after 84 days. Two organizations do not publicly release this information.[41]
- Thirteen of the 28 organizations that publicly report whether they require a woman to be of a specific age before sending her the drugs said there was no age requirement for their organization to send women abortion drugs. Two organizations required girls to be 12 or older, one required girls to be 14 or older, two required girls to be 15 or older, and three required girls to be 16 or older. Seven of the organizations required women to be 18 or older to obtain abortion drugs from their organizations. Ten organizations did not publish this information.[42]
- Of the 29 organizations that publicly report whether their organization requires women to participate in a pre-abortion, synchronous video session to discuss their eligibility for taking the abortion drugs, risks of taking the drugs, etc., 17 required such a video call to take place. Six did not require a video call, and five did not require a video call but made the option available for women who had questions they wanted to ask a provider associated with the organization. One organization made a video call available to a woman depending on what tier of “service” she paid for. Nine organizations did not report this information.
- Of the 23 organizations that publicly reported whether a telephone number was made available to women who were being sent abortion drugs for medical questions, 21 did provide a number, and one did not. One organization made a telephone number available to a woman depending on what tier of “service” she paid for. Fifteen didn’t publicly report this information.
- Nine of the organizations allowed for the advanced provision of abortion drugs to women who were not pregnant at the time they requested the drugs, while 15 did not. Fourteen organizations did not report whether they did or not.
- Of the seven organizations that reported whether they required a woman to provide a form of identification when she was requesting the abortion drugs, four required an ID, and three did not. Thirty-one organizations did not publicly report this information.
- Ten hybrid-and-brick mortar centers ship abortion drugs into states where they physically do not have a location.
- For the step-by-step process of ordering abortion drugs, as well as the questions that the public-facing intake forms asked (if any), see the chart for hybrid brick-and-mortar centers in Appendix C, Table 2.
- Five hybrid brick-and-mortar centers do not require a woman to follow up virtually seven to 14 days after completing the abortion drug regimen, while 10 centers do. Twenty-three centers do not publicly disclose this information on their website.
Findings – Online abortion-drug providers that operate outside of the formal U.S. healthcare system and mail abortion drugs into the country
1. International Online Organizations (3 total)
- Two of the organizations ship abortion drugs into any U.S. state, while Telefem Mexico requires U.S. women to pick up their abortion drugs along the U.S.-Mexico border.
- One of the organizations complied with the REMS requirement that abortion drugs not be prescribed and dispensed after 70 days of gestation. One organization stopped prescribing/shipping abortion drugs to women after 77 days of gestation, and one after 98 days.
- One of the organizations does not require an age requirement for women to request abortion drugs, one requires girls to be 16 or older, and one requires women to be 18 or older.
- None of the three organizations requires a video call before abortion drugs are dispensed to women via the mail, provided the organization determines she is medically eligible to receive the drugs.
- Two of the organizations do not provide a telephone number for women to call if they experience complications after taking abortion drugs shipped by their organization, but they do offer an “online help desk” service staffed by an AI chatbot. One organization does provide a contact number.
- Two of the organizations allow for the advanced provision of the abortion drug regimen, while one doesn’t publicly report that information.
- Two of the organizations do not require women to submit a form of identification before obtaining the abortion drugs, while one (Telefem Mexico) implicitly requires women to present an ID because one needs to show an ID at the U.S.-Mexico border.
- For the step-by-step process of ordering abortion drugs, see the chart for international online organizations in Appendix C, Table 3.
2. E-commerce websites (18 total)
- All 18 websites allow women of any gestational age to buy abortion drugs on their websites. This means that none of them comply with the REMS requirement that abortion drugs be prescribed/shipped no later than 70 days of gestation. Some e-commerce websites, such as Pill Pulse, include phrases on the pages for certain abortion drugs such as “for the non-surgical termination of intrauterine pregnancy up to 63 days (9 weeks) of gestation.” However, the websites do nothing to confirm or formally require that a woman prove she is under a certain gestational age.
- Of the 18 e-commerce websites, seven require a prescription before shipping abortion drugs ordered by women, five do not require a prescription, and six claim they may require one.[43]
- The location where these websites are based versus where they ship abortion drugs from differs. To see more about the locations of these websites, see Appendix C, Table 4, and Appendix A for the locations where the abortion drugs are manufactured for each website.[44]
- Of the 18 e-commerce websites, 16 do not require women buying abortion drugs to consult with a healthcare professional before buying the drugs. One website (Panda Healthcare) states that women have the option to consult with a healthcare professional, and one (Abortion Pills Rx) requires women to fill out a medical eligibility intake form before they can purchase the abortion drugs.
- Of the 18 e-commerce websites, nine do not offer additional medical support if the woman experiences post-abortive complications from abortion drugs ordered on their website. Nine websites offer a live AI chatbot feature that claims to help women with post-abortive complications.
- Of the 18 e-commerce websites, 15 allow women and girls of any age to order abortion drugs from their websites. Three websites state that women have to be 18 or older before ordering abortion drugs off their website.[45]
- Of the 18 e-commerce websites, none required women to present an ID before ordering abortion drugs.
- Of the 18 e-commerce websites, 13 websites’ ordering processes do not allow or require any interaction between the person ordering abortion drugs and a medical professional. One website (Life Easy on Pills) claims women ordering abortion drugs can make a virtual appointment with a gynecologist associated with the organization, but there is no way to schedule an appointment on their website. Four websites claim women interact with the websites’ associated medical professionals because they have to submit a prescription to order the abortion drugs.
3. Community networks (5 total)
- None of the five community networks requires a woman to:
- Have a prescription for abortion drugs from a certified prescriber.
- Consult with a healthcare professional before the network sends her abortion drugs or interact with a doctor at any point in the ordering/request process.
- Meet a certain age requirement before the network sends her abortion drugs.
- Submit an ID before the network sends her abortion drugs.
- None of the community networks has a stated gestational limit at which they will stop sending abortion drugs to women.
- All five community networks are based in the United States but source their drugs from overseas.
- Four of the community networks claim to offer “virtual companion” services, and one (AccessMA) states that they automatically assign a companion to women obtaining abortion drugs from their network after a certain gestational age. The companion service provides women with “support” via phone, text, or email, depending on the network. However, these companions obviously do not provide women suffering from post-abortive complications with any medical care. One network, DASH, claims to offer women medical and emotional support during the abortion via the Signal app, but not after.
- All five of the community networks claim to require women to provide the date of their last menstrual period and/or a positive pregnancy test in their email request for abortion drugs. Theoretically, because of this requirement, women wouldn’t be able to request abortion pills for the future (advanced provision) if they were not pregnant at the time of the request. However, four of these networks do not require women to submit their requests for abortion drugs through a formal medical eligibility intake form using reputable telemedicine platforms. Therefore, there is no way to guarantee that women aren’t making up dates to obtain abortion drugs for the future. One network, AccessMA, has a semi-formalized online intake form. See Appendix C, Table 5 for more details.
Overview of REMS Compliance (or lack thereof) for Each Known Website that Provides American Women with Abortion Drugs
Besides conducting a review of every online abortion-drug provider listed on Plan C and found through other research, CLI reviewed each of these providers’ websites to see if they complied with the REMS requirements that apply to all online abortion-drug providers. In order to capture all of the REMS requirements for online abortion-drug provision, CLI reviewed all of the available forms associated with Mifeprex and the FDA’s webpage on the most current requirements. CLI identified four categories (with subcategories within these) of REMS requirements for Mifeprex: 1) prescriber requirements, 2) patient requirements, 3) dispenser requirements, and 4) general REMS requirements. For tables with the in-depth findings, see Appendix D for each type of online abortion drug provider. Below, the findings of this search and overview are summarized and discussed for each type of online abortion drug provider.
FDA REMS Compliance Findings: Telehealth abortion-drug providers that operate within the formal U.S. healthcare system and mail abortion drugs to women around the country
Prescriber Requirements for Mifeprex
- None of the virtual-only organizations or hybrid brick-and-mortar centers publicly disclose whether their organizations utilize certified prescribers; if their prescribers can assess the gestational age of pregnancies and ectopic pregnancies; if their prescribers can arrange follow-up care if women experience post-abortive complications; or if prescribers are required to sign/read the FDA’s patient agreement form alongside the patient and inform the patient about the risks of the abortion drugs.
Patient Requirements for Mifeprex
- Of the 42 virtual-only organizations, five organizations’ websites say that they require patients to sign and read the FDA’s patient agreement form. Thirty-seven organizations’ websites don’t disclose whether they follow this particular REMS requirement. Of the 38 hybrid brick-and-mortar centers, four centers’ websites say that they require patients to sign and read the FDA’s patient agreement form. Thirty-four websites don’t disclose whether they follow this particular REMS requirement.
Dispenser Requirements for Mifeprex
- None of the virtual-only organizations or hybrid brick-and-mortar centers publicly disclose if the pharmacies they utilize (if they do utilize a pharmacy) have completed a pharmacy agreement form, if the pharmacies provide women with tracking information after the prescription has been filled by the pharmacy, or if the pharmacies dispense pills four days or more after getting a prescription from a certified prescriber only if they have confirmed doing so is safe with the certified prescriber.
General REMS Requirements for Mifeprex
- Thirty-five of the 42 virtual-only organizations prescribe abortion drugs past the FDA’s 70-day limit. Six do follow the FDA’s gestational age limit, and one organization’s website doesn’t say. Twenty-eight of the 38 hybrid brick-and-mortar centers prescribe abortion drugs past the FDA’s 70-day limit, while eight follow the FDA’s gestational age limit. Two of the centers do not publicly disclose this information on their websites.
- Four virtual-only organizations’ online intake forms screen for all the contraindicated conditions for Mifeprex (as laid out in Danco’s medication guide for Mifeprex), while 38 organizations do not publicly disclose this information. Four hybrid brick-and-mortar centers’ online intake forms screen for all the contraindicated conditions for Mifeprex, while 34 centers do not publicly disclose this information.
FDA REMS Compliance Findings – Online abortion-drug providers that operate outside of the formal U.S. healthcare system and mail abortion drugs into the country
None of the organizations and/or websites that compose the three categories of online abortion drug providers operating outside of the formal healthcare system (international online organizations, e-commerce websites, or community networks) meet any of the REMS requirements within the prescriber, patient, dispenser, or general REMS categories of requirements. The overarching commonality is that these providers do not provide U.S. women with Mifeprex or the generic versions (mifepristone) of the drug manufactured by GenBioPro or Evita Solutions (even if their websites claim to), which are the only abortion drugs that are REMS-compliant according to the FDA.[46] As noted above, the FDA specifically considers foreign-sourced abortion drugs to be outside of the FDA-approved supply chain and as such unsafe. For tables with the in-depth findings, see Appendix D for each type of online abortion drug provider operating outside of the formal U.S. healthcare system. More details for each type of online abortion drug provider and their noncompliance with all four categories of REMS requirements are provided below.
Prescriber Requirements[47]
- The international organizations Abortion Pills in Private and Telefem Mexico do not use U.S.-licensed prescribers, so they can’t be considered certified mifepristone prescribers by the FDA. E-commerce websites and community networks don’t utilize any healthcare providers, so they can’t utilize certified prescribers.
- Because the two international organizations described above, e-commerce websites, and community networks do not utilize certified prescribers, they do not utilize certified prescribers who can assess the duration of a pregnancy or ectopic pregnancies, or arrange for follow-up care in the case that a woman suffers from post-abortive complications.
- Because international organizations, e-commerce websites, and community networks do not utilize certified prescribers, they do not use certified prescribers who sign/read the FDA’s patient agreement form with the patient or inform patients of the risks associated with mifepristone. Furthermore, none of the online abortion drug providers sell/ship FDA-approved drugs, so the REMS- associated forms are not part of the requesting or ordering process. Lastly, e-commerce websites don’t require any provider interaction whatsoever, nor does the person ordering the drugs sign any type of consent form.
Patient Requirements
- Because international online organizations, e-commerce websites, and community networks do not provide women with FDA-approved abortion drugs, U.S. women receiving those drugs are unable to sign/read the patient agreement form associated with the drugs they are receiving.
Dispenser Requirements
- Because international online organizations, e-commerce websites, and community networks do not provide women with FDA-approved abortion drugs, the pharmacies (if utilized at all) dispensing abortion drugs to U.S. women are not able to complete the pharmacy agreement form associated with the only FDA-approved drugs.
- Technically speaking, pharmacies (if) utilized by these three types of online abortion-drug providers often provide women requesting/buying the abortion drugs with tracking information for their orders. However, the fact that these three types of providers sometimes satisfy this one dispenser requirement does not minimize the fact that they do not meet any of the other REMS requirements mandated by the FDA. Furthermore, because the tracking information is not for FDA-approved drugs, the table in Appendix D marked none of these providers as satisfying the tracking information sub-requirement.
- Because international organizations, e-commerce websites, and community networks do not utilize certified prescribers, if pharmacies are utilized by these three types of online abortion-drug providers, the pharmacies cannot confirm that dispensing abortion drugs four days or more after receiving a prescription is safe with a certified prescriber. Furthermore, most e-commerce websites and all of the community networks do not require prescriptions in the first place.
General FDA REMS Requirements
- Technically speaking, Telefem Mexico stops providing abortion drugs after women are at more than 70 days of gestation. However, because the drugs Telefem Mexico allows U.S. women to pick up on the U.S.-Mexican border are not FDA-approved, the table in Appendix D marks Telefem Mexico as not satisfying this general FDA requirement. The other two international organizations, Women on Web and Abortion Pills in Private, send non-FDA-approved abortion drugs past 70 days of gestation.
- International organizations, e-commerce websites, and community networks do not require women to complete follow-up appointments to confirm a completed abortion after the women take abortion drugs sent by their respective providers.
- Because international organizations, e-commerce websites, and community networks do not provide U.S. women with FDA-approved abortion drugs, they do not follow the requirements listed in the FDA’s medication guide for screening for contraindications to Mifeprex/mifepristone.[48] Furthermore, e-commerce websites and community networks don’t require women to fill out any medical eligibility forms, so they automatically don’t meet this REMS sub-requirement.
Previous FDA Enforcement Actions Against Certain Online Abortion Drug Providers
As noted in a previous section, federal law (21 U.S.C. §§ 331(a), 331(d), 355(a)) prohibits the importation of misbranded (and unapproved) drugs into U.S. interstate commerce. Several international organizations and e-commerce websites unlawfully misbrand their abortion drugs as FDA-approved, violating yet another federal law. There is historical evidence for this claim alongside evidence from current e-commerce websites. In 2019, the FDA issued warning letters to former international online organizations Aid Access and Rablon for illegally selling misbranded and unapproved mifepristone into the United States. The letters demanded that the two organizations cease the sale of unapproved and misbranded drugs to U.S. consumers and correct all of their other violations of the FFDCA. Rablon is defunct, while Aid Access transitioned to operating within the formal healthcare system in July 2023 and is now considered to be a virtual-only telehealth abortion provider that provides U.S. women with only FDA-approved drugs. Furthermore, in March 2019, the FDA’s Office of Regulatory Affairs Health Fraud Branch issued abuse complaints to registrars of five domain names (with some operating multiple websites) for selling unapproved and misbranded abortion drugs to U.S. consumers.[49] The table below shows which e-commerce websites that received abuse letters in 2019 are still operational as of May 2026.
Table 1 – Current Status of E-Commerce Websites that Received Abuse Letters in 2019 from the FDA’s Health Fraud Branch for Selling Unapproved and Misbranded Abortion Drugs

Of the 28 websites implicated in the FDA’s 2019 abuse letters, 10 are still actively breaking U.S. federal law by selling unapproved and misbranded abortion drugs they claim are FDA-approved. Of those 10 websites, one (Abortionrx.com) is listed on Plan C. Through additional research, CLI found that one other e-commerce website (Birth Control Pills 247) did not receive an abuse complaint in 2019 but is currently sending and selling unapproved drugs that they are claiming are FDA-approved, but are not. The international online organization Abortion Pills in Private is also selling misbranded abortion drugs that they claim are FDA-approved. For screenshots of all 13 of the currently operating e-commerce websites (and Abortion Pills in Private) selling misbranded drugs, see Appendix E. The screenshots and the corresponding websites they come from either represent misbranded abortion drugs that claim to be FDA-approved or engage in other deceptive marketing practices.[50] Reviewing Appendix A shows that all 17 e-commerce websites that disclose which products they sell sell/ship unapproved abortion drugs into the U.S., regardless of whether they misbrand the drugs and/or their website as FDA-approved or certified.[51]
Previous research has further highlighted the quality concerns of buying abortion drugs from e-commerce websites and reported similar findings to the author’s regarding the process of buying such drugs through these websites. A peer-reviewed study published in April 2018 explored the process and feasibility of buying abortion drugs from 18 e-commerce websites that sold non-FDA-approved versions of Mifepristone and Misoprostol to women in the U.S. Twenty-two products were ordered from the 18 identified websites: 20 mifepristone-misoprostol combipacks and two packages of misoprostol-only. The researchers received 18 of the 20 ordered combipacks and both of the packages of misoprostol-only. The study also tested the samples they received in a laboratory to determine the amount of active ingredients in the individual abortion drug tablets. The websites were identified through convenience sampling, meaning that some are no longer in service due to the ephemeral nature of such informal websites. However, half of the websites identified in the study are still actively selling non-FDA-approved abortion drugs.[52] The 2018 study identified several data points relevant to this paper’s findings of false advertising on e-commerce websites:
- The two combipacks that were not delivered to the researchers were bought from two active e-commerce websites—buyabortionpills.net and safeabortionpillrx.com.
- All of the misoprostol pills assayed (200 mcg each) contained some misoprostol. However, the amount per tablet varied from 34.1 mcg to 201.4 mcg.[53]
- None of the websites required the researchers to provide a prescription to order abortion drugs. However, of the nine active websites identified in this study, five say they may require a prescription, and four state they require a prescription to order abortion drugs.[54]
- None of the products received came with instructions or any other written communications. Furthermore, while two websites required completion of an online medical history questionnaire, there were no questions about gestational age or contraindications listed in Mifeprex’s package insert.
- “Few” blister foil packs received by the researchers matched the photo used to advertise the products on the websites.
- Of the eight combipacks that had pinprick holes in them upon delivery, one came from an active website (birthcontrolpills247.com).[55]
Due to the widespread unreliability and illegality of e-commerce “pharmacy” websites like those selling abortion drugs, the FDA launched a campaign in 2018 warning U.S. consumers about the dangers of ordering drugs online and how to safely purchase actual medicine from reputable websites. The campaign, BeSafeRx, was last updated in 2020 and provides resources for health care professionals, consumers, and the media to help people distinguish trustworthy and safe online pharmacies from those that are neither safe or trustworthy.[56] The campaign says that an online pharmacy is likely safe (and unsafe if the opposite is true) if it:
- Always requires a doctor’s prescription
- Provides a physical address and telephone number in the United States
- Has a licensed pharmacist on staff to answer questions
- Is licensed with a state board of pharmacy
The campaign expressly notes that 95% of websites selling prescription medicine online (which would include those selling abortion drugs) are unsafe and unlicensed, and that roughly 5% of those websites comply with U.S. pharmacy laws and practice standards.
Conclusion
Several themes emerged from the findings of this paper related to the legal and regulatory framework surrounding online abortion drug provision. Of the available online abortion drug providers, those operating inside the formal U.S. healthcare system provide more oversight of women ordering abortion drugs than the online sources operating outside of the U.S. healthcare system. The provision of abortion drugs outside of the formal U.S. healthcare system could be characterized as the wild west, as almost zero safeguards exist for women ordering abortion drugs from international online organizations, e-commerce websites, or community networks. However, even telehealth providers operating within the U.S. healthcare system do not provide the type of oversight typically associated with telemedicine or even telehealth services.
While it is unknown whether a majority of telehealth abortion providers operating inside the U.S. healthcare system are compliant with the FDA’s REMS requirements for mifepristone, it is clear that sources operating outside of the healthcare system are not. Among all these sources sending unapproved abortion drugs into the United States, perhaps e-commerce websites are the boldest in the flouting of American laws. Nine active e-commerce websites currently sell abortion drugs they claim are FDA-approved, but are not, and one e-commerce website is engaging in other deceptive marketing practices.
Depending on the source of the online abortion drug provider, the largely uncontrolled online provision of abortion drugs either violates current U.S. laws prohibiting the mailing of abortion drugs within the U.S. or other U.S. laws prohibiting the importation of unapproved and/or misbranded drugs. With the supply and demand for online abortion drugs on the rise, it is time for federal government agencies and Congress, as well as state governments, to seriously consider how the U.S. can simultaneously desire to be seen as a nation of laws, yet willfully turn a blind eye to the current online abortion drug market.
Mia Steupert, M.A., serves as Research Associate at the Charlotte Lozier Institute.
[1] These 13 states include Alabama, Arkansas, Idaho, Indiana, Kentucky, Louisiana, Mississippi, North Dakota, Oklahoma, South Dakota, Tennessee, Texas, and West Virginia.
[2] Only abortion drugs obtained within the formal health care system utilizing telehealth platforms are tracked within the United States. Abortion drugs obtained outside of the formal health care system do not use FDA-approved telehealth platforms and are not tracked by U.S. research organizations such as the Guttmacher Institute and Society of Family Planning (SFP).
[3] These four states include Iowa, Florida, Georgia, and South Carolina. The two states with 12-week laws are Nebraska and North Carolina. Kansas, Ohio, and Wisconsin (22 weeks of gestation); Utah (18 weeks); and Pennsylvania and New Hampshire (24 weeks) limit abortion at differing gestational ages. Fifteen states have ineffective post-viability limits (Arizona, California, Connecticut, Delaware, Hawaii, Illinois, Maine, Massachusetts, Montana, Missouri, Nevada, New York, Rhode Island, Virginia, and Washington) because their laws have such broad health exceptions that abortions after viability can be obtained for virtually any reason. Nine states and the District of Columbia have no gestational limits: Alaska, Colorado, Maryland, Michigan, Minnesota, New Jersey, New Mexico, Oregon, and Vermont.
[4] These states include Florida, Nebraska, and South Carolina. The Rhites Map linked above states that Nebraska has an implicit ban on telehealth abortions, but in an email to CLI in 2025, the Nebraska Department of Health and Human Services stated that telehealth abortions are prohibited in Nebraska. This list of states doesn’t include the states that have explicit prohibitions on telehealth abortions but also completely prohibit the provision of abortion within the state, such as Arkansas.
[5] One of the reasons for such a dramatic increase in the percentage of telehealth abortions as a share of the U.S. total is that #WeCount’s reporting methodology became much more detailed in July 2023. It started including telehealth abortions obtained by women in pro-life states via shield laws for the first time since data collection for the project commenced. However, the majority of the increase can be attributed to legal and regulatory factors.
[6] Mifepristone when discussed in this paper refers to the generic forms of mifepristone manufactured by GenBioPro and Evita Solutions as well as the brand name version Mifeprex, manufactured by Danco, unless the author is specifically referring to a particular sponsor’s drug approval.
[7] This paper will not go into detail about the safety or unsafety of online access to abortion drugs. However, please see the FDA’s 2021 response to a 2019 citizens’ petition filed by pro-life doctors to review the different studies referenced when claiming online access to abortion drugs is safe. Additionally, see this primer containing several studies supporting claims that online access to abortion drugs is unsafe.
[8] The estimates in part two of this paper will most likely change in the months and years to come because they are point-in-time estimates that will change as new organizations and centers open and others close and as other websites and community networks open and close. However, the findings that these estimates represent will likely hold steady barring legal and regulatory changes to online abortion drug access by U.S. federal agencies, Congress, and/or state governments.
[9] The location where Evita Solutions has mifepristone manufactured is unknown.
[10] It is important to note that Charlotte Lozier Institute does not believe that the online provision of abortion drugs in any way or by any type of online provider constitutes true telemedicine or even telehealth, just as CLI does not believe that abortion is healthcare in any sense of the word. The terms “telemedicine” and “telehealth” imply the provision of medicine and healthcare, which abortion by drug-induced means does not provide. Procedures that cause death to another human being should not be considered telehealth, telemedicine, or healthcare in general. The reason why this paper categorizes certain types of online abortion drug access/provision as telehealth is because that is what the existing research, as laid out by government (the FDA) and research organizations, uses, and the purpose of this paper is not to recreate a framework of terminology.
[11] For example, Dr. Margaret Carpenter, a New York-licensed abortion drug provider who mails abortion drugs to women in Texas, is licensed to practice medicine in New York but not in Texas, meaning that if New York, their shield law, and the abortion industry consider the provision of abortion to be medical care, Dr. Carpenter is practicing medicine in Texas without a license. If one looks up Dr. Carpenter on Texas’ Medical License Lookup Tool, no results show up. Similarly, Dr. Remy Coeytaux is a California-licensed doctor who mails abortion drugs into pro-life states like Texas and is associated with the virtual-only organization Aid Access. He is not licensed to practice medicine in Texas.
[12] Drug-induced abortions that fall under this category are also sometimes called “self-managed abortions.” In other contexts, “self-managed abortions” can also mean abortion by other self-managed means with the sole intent of killing an unborn child (i.e., the ingestion of herbs or causing bodily harm to oneself to terminate one’s pregnancy). However, in the context of this paper, “self-managed abortion” refers to abortions carried out via abortion drugs obtained online outside of the formal U.S. healthcare system.
[13] CLI calculated the total number of each type of virtual-only organization by reviewing all the available organizations listed on the Plan C website for this specific type of online abortion drug provider. Also, it is important to note that the 34 organizations that strictly ship abortion drugs within/into pro-abortion states don’t require women to be residents of the states the organizations ship drugs into. They only require that women are physically present in the state where the provider is licensed during the telehealth appointment, and have a mailing address within the state to which the abortion drugs can be shipped. Plan C is often mistakenly listed as an abortion drug provider. Plan C does not ship abortion drugs to women. They are an online directory that shows woman where and how they can obtain abortion drugs based on their state of residence. Information about the websites listed within Plan C’s directory regarding how the different websites/organizations operate came directly from the Plan C website or the organization’s website itself.
[14] CLI utilized the same collection methodology for hybrid brick-and-mortar centers that was laid out in footnote 13.
[15] For example, as laid out in Appendix C, Table 2, 10 of the 38 hybrid brick-and-mortar centers ship abortion drugs into states where they have no physical center.
[16] One of the international organizations, Telefem Mexico, only allows for pickup along the U.S.-Mexico border (on the Mexico side). The organization does not ship abortion drugs to addresses within the United States. The other two international online organizations (Abortion Pills in Private and Women on Web) ship abortion drugs directly to U.S. women. CLI utilized the same collection methodology for international organizations that was laid out in footnote 13. Abortion Pills in Private’s website lists a United Arab Emirates address and phone number and Women on Web is a Canadian nonprofit organization.
[17] See Appendix C, Table 3 for more information.
[18] See Appendix A for how e-commerce websites, despite claiming they sell FDA-approved abortion drugs, sell abortion drugs manufactured by sponsors not approved by the FDA.
[19] To see the different websites and the abortion drugs they offer as well as the drugs’ associated manufacturers, see Appendix A. The information contained within the table in Appendix A was found either on the e-commerce website links for the specific drugs or through this database.
[20] Plan C’s website notes that e-commerce websites “do not require a prescription for the medications, do not require the purchaser to upload an ID, and do not provide a medical consultation or any kind of support.” To see this quote, visit the hyperlink in the previous sentence, scroll down to the section “Websites that sell pills (7),” click on the question mark bubble and then click on the tab, “What are websites that sell pills.” CLI’s findings described later in this paper do differ from Plan C’s statement in that some e-commerce websites seem to require prescriptions. However, CLI’s findings corroborated Plan C’s claim about the lack of medical support and requirement to upload an ID when ordering abortion drugs.
[21] Plan C lists e-commerce websites that meet their quality control criteria (which they don’t publish publicly). Their website states, “The pills were real (based on laboratory testing). But we do not operate these sites, and cannot guarantee they will be reliable in the future.” To see this quote, visit the hyperlink in the previous sentence, scroll down to the section “Community networks (1)” click on the question mark bubble and then click on the tab, “What are community networks.” As noted in Appendix C, Table 4, there are several e-commerce websites that aren’t listed on Plan C’s website but were discovered by the author through additional research. Relatedly, Plan C notes on their website that these e-commerce websites “sell pills but do not include any additional support …They sell generic abortion pills that are not regulated or inspected by the US government.”
[22] CLI utilized the same collection methodology for community networks that was laid out in footnote 13.
[23] While Red State Access controls the four sub-networks, those subnetworks all have slightly different protocols and offer different emotional “support” services. Furthermore, of the four subnetworks only AccessMA has their own website. Red State Access, unlike the four subnetworks, does not distribute abortion drugs, but rather acts as a logistical and administrative coordinator.
[24] The TelAbortion Study was a multi-year study focused on testing the direct-to-patient model of telehealth abortion that resulted in multiple published peer-reviewed studies detailing the “safety” and efficacy of this model.
[25] CLI discovered that the hybrid brick-and-mortar telehealth abortion services associated with the four Her Smart Choice brick-and-mortar abortion centers in California are the only hybrid brick-and-mortar centers (and the only telehealth abortion provider operating inside the formal U.S. healthcare system) that utilizes the direct-to-patient model requiring in-person, pre-abortion ultrasounds and bloodwork. Drugs are still dispensed via the mail, but these centers do not utilize a no-test model of telehealth abortion.
[26] It is important to note that while this paper does not address the safety or unsafety of mifepristone (Mifeprex) and misoprostol, omitting the mention of the black box warning on Mifeprex would be misleading and provide an incomplete account of the drug’s history. Black box warnings are the highest safety warning imposed by the FDA and are added to drugs associated with substantial safety concerns elicited by significant clinical data. The black box warning was added to Mifeprex’s package insert in 2004 and included a note about a potential for bacterial infections, sepsis, excessive bleeding, and death occurring after the use of Mifeprex. The warning was added to the package insert because of five reports of fatal septic shock following the use of Mifeprex in the U.S. (four reports) and Canada (one report). The official text of Mifeprex’s black box warning, as well as the warning in GenBioPro and Evita Solutions’ package inserts for mifepristone, are included in the form of photographs in Appendix F.
[27] The 2000 approval of Mifeprex included the same limitations that the 2011 REMS formalized. No new regulations were added in 2011. However, the 2000 approval utilized a different statutory framework than REMS uses to place safety restrictions on the drug, Mifeprex. The 2000 statutory framework for mifepristone was part of 21 CFR Part 314 Subpart H. These limitations included prescriber qualifications, limits on where the drug could be dispensed (an in-person requirement), signed patient agreement forms, mandatory reporting of adverse events, and the provision of a patient medication guide. In 2007, the Food and Drug Administration Amendments Act passed. This legislation significantly increased the FDA’s regulatory authority to control post-approval drug safety, and it authorized the current day REMS regulatory framework. In 2011, the 2000 limitations placed on Mifeprex transitioned to the REMS statutory framework created by the 2007 legislation. The REMS requirements described above are the same for all three versions of the abortion drug (Mifeprex, the brand name, and the two generic versions of mifepristone). The linked REMS documents above and below are for the brand name Mifeprex drug. To see the REMS documents for GenBioPro’s generic version of the abortion drug, see the links here.
[28] This is a summary and not an exhaustive list of the original REMS requirements.
[29] The prescriber certification and patient agreement requirements were kept as REMS requirements.
[30] AHM filed this case in November 2022. On April 7, 2023, a federal district court in Texas paused the FDA’s approval of mifepristone. However, the pause was ordered to go into effect in seven days to allow for the former Biden administration to appeal the decision in the appellate courts, so no changes to the drug’s REMS actually occurred. On April 12, 2023, the 5th Circuit Court of Appeals overturned the district court’s pause on the overall approval of mifepristone but required that the in-person dispensing requirement for abortion drugs be reimplemented. Additionally, the April 12, 2023 ruling moved back the permissible gestational age from 10 weeks of gestation (as changed with the 2016 REMS modifications) to seven weeks and repealed other 2016 REMS modifications. On April 14, 2023, the U.S. Supreme Court enacted a temporary stay on the April 7, 2023, district court ruling in its entirety while the case continued to play out in lower courts, meaning that telehealth abortions remained legal and other changes to the 2023 REMS were paused. Several Supreme Court orders extended its earlier temporary stay. On August 16, 2023, the 5th Circuit Court of Appeals ruled that the FDA must restore mifepristone’s in-person dispensing requirements as well as the other requirements laid out in the court’s April 12, 2023, ruling. However, due to the Supreme Court’s earlier stay on changes to abortion drug access, mifepristone remained available under the 2023 REMS regulations. On June 13, 2024, the U.S. Supreme Court ruled that AHM lacked legal standing to challenge the FDA’s REMS for Mifepristone and reversed the 5th Circuit Court’s ruling, meaning that telehealth abortions would remain legal and accessible across the country.
[31] See Table 1 for which active e-commerce websites are shipping unapproved abortion drugs into the U.S., Appendix A for where the unapproved drugs are manufactured and by whom, and Appendix E for which websites erroneously advertise their abortion drugs as FDA-approved.
[32] These 14 states include Arizona, Connecticut (and Public Act No. 22-19, 2022), Delaware, Hawaii, Illinois, Maryland, Michigan (and Executive Directive No. 2022-5), Minnesota, Nevada, New Jersey (and N.J. Stat. §2A:84A-22.19), New Mexico, North Carolina (and Executive Order No. 8, 2025), Oregon, and Pennsylvania. Arizona, Michigan, North Carolina, and Pennsylvania enacted shield laws via executive order while the remaining states and D.C. enacted their shield laws via legislation.
[33] The eight states include California, Colorado, Maine, Massachusetts, New York, Rhode Island (and S2262 Substitute B, 2024), Vermont, and Washington. For six of these eight states’ shield laws (CO, ME, MA, NY, RI, and VT) the law requires that the shielded abortionist be licensed to perform abortions in the shielding state and physically reside in the shielding state. California and Washington’s shield laws only specify that the shielded “provider” be licensed to perform abortions in the shielding state. For more information on these eight shield laws, see Appendix B.
[34] To arrive at these calculations, please utilize the #WeCount data explorer tool and add the 12 monthly totals obtained by filtering for the entirety of 2024 as well as by abortion provided under shield laws to states with: telehealth restrictions, 6-week laws, and total bans.
[35] This section will not cover in detail the Alliance for Hippocratic Medicine (AHM) v. U.S. Food and Drug Administration case because it was decided in June 2024 and ultimately dismissed because of AHM’s lack of standing. While the case mainly focused on the abortion drug regimen in general, the plaintiff argued that the in-person dispensing requirement should be reinstated.
[36] See the beginning of the paper for a case update.
[37] The organizations rely on the patient’s self-reported date for the first day of their last menstrual period (LMP) and/or the patient’s self-reported date for their positive pregnancy test.
[38] It is unclear how the organizations that have age requirements confirm the age of the woman requesting abortion drugs since a majority of the websites with age requirements didn’t publish information on if they required women to submit an ID before being provided with abortion drugs.
[39] In late 2024, an Ohio surgical resident at the University of Toledo, Hassan-James Abbas, ordered abortion drugs from an out-of-state provider using his estranged wife’s information (without her consent) to abort the pregnancy of his then-girlfriend. Abbas used his estranged wife’s name, date of birth, and driver’s license number, but his own credit card information, email, and delivery address. The identity/category of the online abortion drug provider used by Abbas was not publicly disclosed. The girlfriend wanted to keep the unborn child, but one night in December 2024, she woke up to Abbas on top of her, forcing the crushed-up abortion drugs inside her mouth. As a result of this coerced abortion and other ensuing crimes, the state of Ohio suspended Abbas’ medical license and he is now facing criminal charges and has been formally indicted. This horrifying anecdote highlights how even websites that seemingly require those ordering abortion drugs to submit identifying information (often in the form of an ID) are often unable to confirm the actual identity of those ordering the drugs and detect abortion coercion and instances of domestic violence.
[40] It is unclear how these networks’ intake forms, or intake forms generated by any of the organizations and/or websites mentioned in this paper, guarantee the person ordering abortion drugs is not making up a gestational age or LMP, or any other information they enter into the intake form.
[41] The organizations rely on the patient’s self-reported date for the first day of their last menstrual period (LMP) and/or the patient’s self-reported date for their positive pregnancy test. Additionally, the FDA has admitted that the requirement that drug-induced abortions take place within 70 days of gestation should theoretically prohibit the advanced provision of abortion drugs because, as Patrizia Cavazzoni, then-Director of the Center for Drug Evaluation and Research (CDER) at the FDA, noted in a 2021 letter, “…patients who are not pregnant at the time of evaluation would not be appropriate candidates for being prescribed mifepristone for medical termination of pregnancy because they do not fulfill the approved indication of having an intrauterine pregnancy of up to 70 days gestation.”
[42] It is unclear how most of the organizations with age requirements confirm the age of the woman requesting abortion drugs. Only two of the organizations with age requirements publicly disclose that they require women to submit an ID before receiving abortion drugs (FPA Women’s Health and Scotsdale Women’s Center). Furthermore, two of the organizations (UCLA OB/GYN and Blue Mountain Clinic) with supposed age requirements do not require women to submit an ID, so the organizations are depending on a woman’s self-reported age. The unreliability of submitting identifying information online also speaks to the larger issue of the unreliability of online intake forms in general, regardless of the type of online abortion provider.
[43] It is unclear for the seven websites that supposedly require a prescription how they enforce this, because one can check out on all eight websites without submitting a prescription.
[44] As noted in Appendix A, several websites advertise their abortion drugs as mifepristone and misoprostol. While the drugs may have the same chemical properties as the FDA-approved versions of Mifepristone and Misoprostol, they are not the same as the FDA-approved versions of the drug (despite claiming they are) in that they are not sponsored by the FDA-approved manufacturers for these drugs. This is why these e-commerce websites have been accused of selling misbranded abortion drugs.
[45] It is unclear how the three websites enforce this requirement because none of them require a form of ID to be submitted before buying abortion drugs.
[46] Even if these e-commerce websites somehow obtained abortion drugs from FDA-approved sponsors, the websites still would not be following the FDA’s REMS requirements because they are not certified prescribers or pharmacies.
[47] Women on Web’s online intake form claims that abortion drug requests from women located in the U.S. are fulfilled by U.S. based doctors. However, it is unclear if these doctors are certified prescribers/dispensers. Relatedly, Women on Web seems to use a dispenser that is not REMS certified. As this Catholic Register article notes, the abortion drugs mailed by Women on Web are produced by the Indian company Synokem and brought to market by DKT India. In other words, they provide U.S. women with non-FDA approved drugs from a non-REMS certified drug sponsor (Synokem).
[48] Some e-commerce websites, such as Buy Abortion Pills, list some of the contraindications enumerated in the medication guide for Mifeprex, but the websites do nothing to screen women buying abortion drugs for those contraindications.
[49] The five letters can be found here: Rebel Ltd; NameCheap, Inc.; Crazy Domains/Dreamscape Networks FZ-LLC; Public Domain Registry; and Communigal Communication Ltd.
[50] Appendix E contains a single screenshot for each website selling misbranded abortion drugs, not a picture for every instance that each website sells misbranded drugs because almost all of the abortion drugs on these websites are misbranded in that they say the drugs are FDA-approved.
[51] Some of the websites listed in Appendix A advertise that they sell FDA-approved products. However, it is still illegal to buy abortion drugs from these pharmacies because they are either foreign pharmacies and violate the Federal Food, Drug, and Cosmetic Act (FFDCA) (Section 801(d)(1)(B)) or are U.S.-based pharmacies that are selling prescription drugs without requiring the purchaser to have a prescription.
[52] These nine websites include abortionrx.com, onlineabortionpillrx.com, nopregnancy.com, daynighthealthcare.com, abortionpillrx.com, abortionpillsrx.com, birthcontrolpills247.com, buyabortionpills.net, and safeabortionpillrx.com.
[53] The study found that all mifepristone pills received contained mifepristone in amounts within 8% of the stated amount (200 mg).
[54] The five websites include abortionrx.com, abortionpillrx.com, abortionpillsrx.com, buyabortionpills.net, and safeabortionpillrx.com. The four websites include onlineabortionpillrx.com, nopregnancy.net, daynighthealthcare.com, and birthcontrolpills247.com. It is important to note that this study was published in 2018, and theoretically the websites could have implemented an actual prescription requirement.
[55] The product ordered from this active website, a Pregnot kit, seems to not be advertised on the website anymore.
[56] The FDA’s use of the word “pharmacy” is different from the use of the term on e-commerce websites that sell abortion drugs and claim to be an online pharmacy.














