










Hyde @ 40: Analyzing the Impact of the Hyde Amendment with July 2020 Addendum

This is Issue 61 of the On Point Series. The most current version of this paper can be found at Hyde @ 40: Analyzing the Impact of the Hyde Amendment with July 2020 and June 2023 Addenda, On Point 96.
Introduction
This paper provides a history of the Hyde Amendment and summarizes the substantial body of academic and policy research which shows that the Hyde Amendment lowers abortion rates. It uses this research to estimate the number of lives saved by the Hyde Amendment since it was first signed into law in 1976. Our estimates indicate that as of July 2020, the Hyde Amendment has saved approximately 2,409,311 lives.
Editor’s Note (6/27/2023): This paper has been updated to include calculations through May 31, 2023. For the most current paper, please see: https://lozierinstitute.org/hyde-40-analyzing-the-impact-of-the-hyde-amendment-with-july-2020-and-june-2023-addenda/
Addendum to Hyde @ 40:
Analyzing the Impact of the Hyde Amendment
Originally published July 2020
Since the Charlotte Lozier Institute’s analysis of the Hyde Amendment was published in November of 2016, three states have changed how their Medicaid programs cover elective abortions.
Maine
At various points in the 1970s, Maine funded elective abortions though its Medicaid program. However, it quit funding elective abortions through Medicaid after the U.S. Supreme Court’s Harris v. McRae decision in 1980.[1] As of 2016, the federal Hyde Amendment was saving approximately 352 lives a year in Maine. However, in June of 2019, Maine Governor Janet Mills signed legislation that required that required the state to fund all elective abortions for Medicaid-eligible women. This piece of legislation took effect September 19, 2019.[2] Therefore, I estimate the Hyde Amendment saved approximately 282 lives in Maine in 2019 and no lives in 2020.
Illinois
After the U.S. Supreme Court’s 1980 Harris v. McRae decision, Illinois did not fund elective abortions through its state Medicaid program.[3] In 1994, the Circuit Court of Cook County held that the state’s abortion funding limits violated the state constitution. However, in practice, Illinois still did not fund elective abortions through its state Medicaid program.[4] As of 2016, the federal Hyde Amendment was saving approximately 3,918 lives per year in Illinois. In September of 2017, Illinois Governor Bruce Rauner (R) signed HB 40, which mandated taxpayer funding of abortion for low-income women through Medicaid. This law took effect on January 1, 2018.[5] Because of this, the Hyde Amendment did not save any lives in Illinois in 2018, 2019, and 2020.
West Virginia
During the 1970s, West Virginia began funding elective abortions through its state Medicaid program; [6] the federal Hyde Amendment had no impact on the incidence of abortion in West Virginia. However, on November 6, 2018, West Virginia voters approved Amendment 1 to their state constitution. This amendment specifically prevents taxpayer funding of elective abortions through the state Medicaid program. Since Amendment 1 took effect immediately upon its approval,[7] I estimate that it has saved approximately 835 lives since 2018.[8]
Summary
Because of these public policy changes that have taken place since November of 2016, the Hyde Amendment is now protecting unborn children in West Virginia. However, it is no longer protecting them in Illinois and Maine. Since the number of women of childbearing age who reside in Illinois and Maine exceeds the number of women of childbearing age who reside in West Virginia, the overall impact of the Hyde Amendment has been slightly diminished. I estimate that the Hyde Amendment saved 63,549 lives in 2016; 63,549 lives in 2017; 59,707 lives in 2018; 60,067 lives in 2019; and 29,713 lives in 2020 (as of July 1). Overall, I now estimate that the Hyde Amendment has saved a total of 2,409,311 lives since 1976.
[1] Merz, Jackson, and Klerman. 1995. “A Review of Abortion Policy: Legality, Medicaid Funding, and Parental Involvement, 1967-1994” Women’s Rights Law Reporter 17 (1) 1-61.
[2] https://bangordailynews.com/2019/10/30/news/maine-laws-expanding-abortion-access-unlikely-to-fill-federal-funding-gap-providers-say/
[3] Merz, Jackson, and Klerman. 1995.
[4] Merz, Jackson, and Klerman. 1995.
[5] https://www.chicagotribune.com/news/ct-illinois-abortion-timeline-htmlstory.html
[6] Merz, Jackson, and Klerman. 1995.
[7] https://www.theintelligencer.net/news/top-headlines/2018/11/amendment-1-has-passed-what-now/
[8] Specifically, we predict it saved 77 lives in 2018, 507 lives in 2019, and 251 in 2020 (as of July 1).
Hyde @ 40:
Analyzing the Impact of the Hyde Amendment
Originally published September 2016
Executive Summary
- Over 20 studies in a variety of peer-reviewed academic journals demonstrate the Hyde Amendment and other laws to limit public funding of abortion reduce abortion rates and protect unborn children.
- Multiple studies show that when the Hyde Amendment took effect, the birthrate among women on Medicaid increased by an average of about 13 percent. That means in U.S. states that do not fund abortion through Medicaid, one in every nine people born to a mother on Medicaid owes his or her life to the Hyde Amendment.
- Since 1976, the best research indicates that the Hyde Amendment has saved over two million unborn children.
*The author would like to thank Charlotte Lozier Institute intern Sally Fowler for her excellent work as a research assistant this summer.
Introduction
Congress enacted the first Hyde Amendment on September 30, 1976. It was named after its sponsor Congressman Henry Hyde (R-IL) and was a rider to the annual HHS Labor appropriations bill. The Hyde Amendment has been passed every year since 1976 and has largely prevented federal Medicaid dollars from paying for abortions. The Hyde Amendment has played an important role in the history of the national debate on abortion. Its passage was one of the pro-life movement’s first major legislative victories. Additionally, the Supreme Court’s Harris v. McRae decision in 1980, which upheld the Hyde Amendment, was one of the pro-life movement’s first judicial victories Scholars and analysts from a range of ideological perspectives agree that the Hyde Amendment has had a significant impact on the incidence of abortion in the United States. As such, now is an apt time to look back on the amendment’s history and analyze its impact during the past 40 years.
History of the Hyde Amendment
As abortion became legal in several states in the late 1960s and early 1970s, policymakers started to grapple with questions about whether and to what extent abortions should be subsidized for low-income women. Evidence indicates that Medicaid reimbursed for eligible women who obtained abortion under those states’ laws. That is, Medicaid originally treated abortion the same as any other medical procedure (Merz, Jackson, and Klerman 1995).
In the late 1960s and early 1970s pro-life lobbying efforts focused on preventing additional states from legalizing abortion and repealing state laws that had legalized abortion. At first he question of public funding for abortion received relatively little attention from pro-life activists. However, after the Supreme Court’s Roe v. Wade decision in 1973, a number of states took steps to restrict payment eligibility under state Medicaid programs. This resulted in a variety of legal challenges, which culminated in the Beal v. Doe, Maher v. Roe, and Poelker v. Doe cases decided by the U.S. Supreme Court in 1977. These cases held that the government is not required to fund elective abortions either under terms of the federal statute or under the U.S. Constitution (Merz, Jackson, and Klerman 1995).
However, throughout the 1970s, the federal government was providing reimbursement for abortions through Medicaid. On September 30, 1976, Congress passed, over a presidential veto the first of a long line of budgetary acts – each subsequently referred to as the Hyde Amendment – restricting federal Medicaid funds for abortions. On the same day, several lawsuits were brought challenging the constitutionality of the Hyde Amendment and a Temporary Restraining Order (TRO) was issued on October 1, barring enforcement of the Hyde Amendment. After a hearing, the district court in McRae v. Mathews entered a preliminary injunction on October 22, 1976. Under the injunction, the federal government continued to fund abortions through 1976 (Merz, Jackson, and Klerman 1995).
Extensive litigation over the constitutionality of the Hyde Amendment continued throughout the 1970s. A trial court dissolved the TRO and starting August 4, 1977 the federal government only reimbursed for abortions performed to save the life of the woman. Starting in February 14, 1978 the Hyde standard was expanded to include abortions in cases of rape, incest, and long-term physical health damage to the woman.
Lower court rulings continued to be appealed and the Supreme Court agreed to rule on the constitutionality of the Hyde Amendment in 1980. On February 19, 1980, the U.S. Supreme Court denied a stay of the injunction and the federal government resumed funding therapeutic abortions. On June 30, 1980, the U.S. Supreme Court upheld the constitutionality of the Hyde Amendment by a 5-4 vote in Harris v. McRae. Federal funding for therapeutic abortions was finally eliminated on September 19, 1980 after the U.S. Supreme Court declined a rehearing in the McRae case (Merz, Jackson, and Klerman 1995). From that time up until October 1, 1993, federal matching funds were available only for abortions performed to save the life of the woman. However, effective October 1, 1993, the federal Hyde standard was extended, providing reimbursement for abortion when pregnancy results from an act of rape or incest (Rovner 2009). Most states altered their state plans to match the federal standard, but many states did not because of state laws, regulations, or constitutional provisions limiting the use of states funds to pay for abortions performed only to save the life of the mother (Merz, Jackson, and Klerman 1995).
Since the Hyde Amendment took effect, the federal government has paid for abortions only under limited circumstances. However, states have always had the ability to pay for or subsidize abortions with their own Medicaid funds. Currently 15 states pay for abortions for low-income women through their state Medicaid program.1 Interestingly, 11 of those 15 states are funding abortion through Medicaid because of a judicial ruling or a court order. Only four states have enacted legislation requiring the government to fund abortion using state-originated funds through Medicaid (Guttmacher Institute 2016).
Impact of the Hyde Amendment
There has been a considerable amount of research on the impact of Medicaid funding restrictions on the incidence of abortion. A 2009 Guttmacher Institute literature review identified 22 studies on this topic (Henshaw et al. 2009). These methodologically diverse studies used abortion data from a variety of sources. Overall, of the 22 studies they considered, 19 found statistically significant evidence that abortion rates fell after Medicaid funding was reduced.
This finding held for studies using time-series cross-sectional data to analyze overall abortion rates (Blank, George, and London 1996; Haas-Wilson 1993; 1997; Hansen 1980; Levine, Trainor, and Zimmerman 1996; Matthews, Ribar, and Wilhelm 1997; Medoff 2007; Meier et al. 1996; Meier and McFarlane 1994). It also held for studies using time-series cross-sectional data to analyze teen abortion rates specifically (Haas-Wilson 1996; Lundberg and Plotnick 1990; Medoff 1999; 2007). This held as well for studies that analyzed abortion rates in smaller groups of states (Korenbrot, Brindis, and Priddy 1990; Trussell et al. 1980) and for two studies that specifically analyzed the impact of public funding restrictions on pregnancy outcomes in Illinois (Sheier and Tell 1980), Texas (Chrissman 1980), and North Carolina (Cook et al. 1999; Morgan and Parnell 2002).
The studies that analyzed data from North Carolina were especially interesting. From 1980 to 1995, North Carolina publicly funded abortion for low-income women—not through Medicaid but through a state abortion fund that periodically ran out of money. Whenever funds were depleted, the researchers found there were statistically significant decreases in the abortion rate, and months later, statistically significant increases in the birthrate (Cook et al. 1999; Morgan and Parnell 2002). These findings were statistically stronger when the pregnancy outcomes for African-American women were considered. Overall, Cook et al. concluded that 37 percent of the women who would have otherwise had an abortion carried their child to term when public funding was not available. Overall, the authors of the Guttmacher literature review acknowledge that the best research indicates that Medicaid funding limits reduce the incidence of abortion. In the discussion that follows the literature review, they state that:
the best studies . . . used detailed data from individual states and compared the ratio of abortions to births both before and after the Medicaid restrictions took effect. These found that 18-37 percent of pregnancies that would have ended in Medicaid funded abortions were carried to term when funding was no longer available. (Henshaw et al. 2009, 27)
They state that the Cook et al. study analyzing data from North Carolina had the “best design.” They conclude by stating that “[c]onsidering the case studies collectively, a reasonable estimate is that a lack of funding influences a quarter of Medicaid-eligible women to continue unwanted pregnancies” (Henshaw et al. 2009, 27). Overall the research paints a clear picture. By limiting public funding for abortion, the Hyde Amendment reduced the incidence of abortion and saved lives.
Analyzing the Overall Impact of the Hyde Amendment
Even though consensus exists that the Hyde Amendment has stopped abortions and saved lives, there is little research on how many lives the Hyde Amendment has actually saved. In 2010, the Center for Reproductive Rights released a report entitled “Whose Choice? How the Hyde Amendment Harms Poor Women.” The report includes a quote by Stephanie Poggi, executive director of the National Network of Abortion Funds, which states that, “Because of the Hyde Amendment, more than a million women have been denied the ability to make their own decisions.” A number of journalists and commentators have used this one million figure in their reporting on the impact of the Hyde Amendment (Nance 2016; Faulkner 2016).
The 2010 Center for Reproductive Rights report cites some studies which show that the Hyde Amendment reduces the incidence of abortion and makes it more likely that a woman on Medicaid will carry her pregnancy to term. However, the report provides absolutely no information about the methodology behind the 1 million figure. Furthermore, when contacted this summer, the Center for Reproductive Rights was unable to provide any information about the methodology used in their 2010 report. They suggested that we contact Stephanie Poggi directly. However, Ms. Poggi no longer works for the National Network of Abortion Funds and could not be reached.
As the Hyde Amendment reaches its 40th anniversary this year, it is worthwhile to have more reliable figures on how many lives it has saved. Methodologically, the best way to analyze the impact of the Hyde Amendment is to look at the impact of Medicaid-funding restrictions on either the abortion rate of women on Medicaid or the birthrate of women on Medicaid. Indeed, three separate studies that analyzed Medicaid recipients in Illinois, Texas, and Ohio found that after the Hyde Amendment took effect, the birthrate among women on Medicaid increased by anywhere from 11 percent to 15 percent. The average increase in the Medicaid birthrate was almost 13 percent.
So if the number of Medicaid births in a given state increased from 1,000 to 1,130 after the Hyde Amendment took effect, 130 people or approximately 11 percent of those born to a mother on Medicaid would owe their lives to the Hyde Amendment. Alternatively, one of every nine people born to a mother on Medicaid in a state not funding abortions through Medicaid owes his or her life to the Hyde Amendment.
This nicely demonstrates the lifesaving impact of the Hyde Amendment. However, obtaining state-level data dating back to the 1970s on the number of women of childbearing age on Medicaid proved to be logistically difficult. A more feasible way to analyze the number of abortions prevented by the Hyde Amendment is to look at the impact of public funding restrictions on either the overall abortion rate (abortions per 1,000 women of childbearing age) or the overall abortion ratio (abortions per 1,000 live births). The abortion rate tends to be a more reliable measure than the abortion ratio. That is because population numbers tend to be fairly stable from year to year, while the birthrate tends to fluctuate. Consequently, analyzing the effect of the Hyde Amendment on the abortion rate is a more reliable way to gauge its impact.
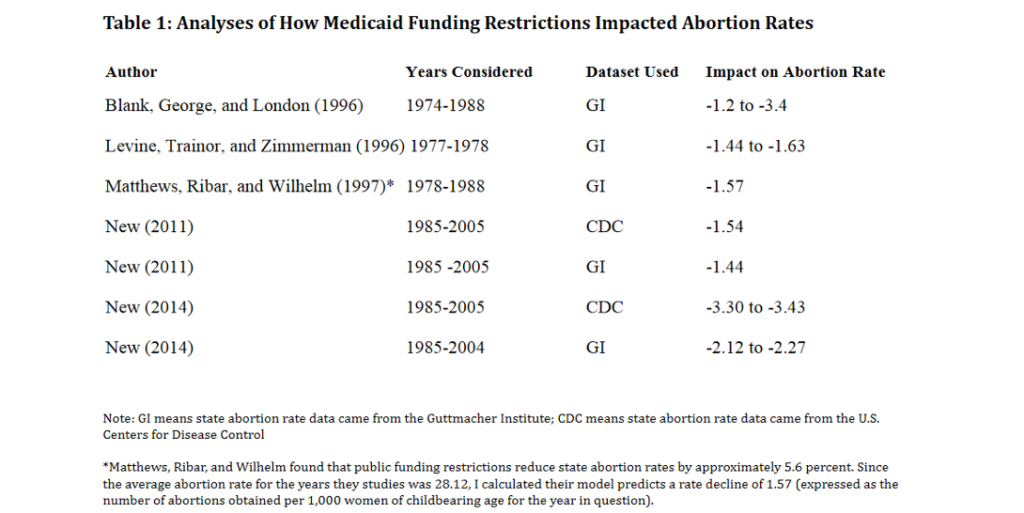
The 2009 Guttmacher Institute literature review on public funding of abortion identified seven peer- reviewed studies which analyzed the impact of public funding restrictions on state abortion rates (Hansen 1980; Haas-Wilson 1993,1997; Meier et al. 1996; Blank, George, and London 1996; Levine, Trainor, and Zimmerman 1996; Mathews, Ribar, and Wilhelm 1997). Two additional academic studies on the subject were published after 2009 (New 2011; New 2014). Unfortunately, some of these studies are limited in their ability to properly analyze the impact of the Hyde Amendment. Two studies only analyze one year of abortion data (Hansen 1980; Haas-Wilson 1993). Another study interacts the Medicaid funding restriction variable with the state poverty rate and hence does not provide a standalone estimate on the impact of Medicaid funding restrictions (Haas-Wilson 1997). Another study looked at the publicly funded abortion rate instead of the presence of public funding as an independent variable (Meier et al. 1996).
That said, the Guttmacher literature review includes three studies which analyzed the impact of public funding restrictions on state abortion rates for an extended period of time. My two State Politics and Policy Quarterly studies also analyzed state abortion data for a span of 20 years. Table 1 lists each of these five studies, the datasets they used, the years that were analyzed, and their findings on how public funding restrictions impacted abortion rates. The results indicate that Medicaid funding limits reduce state abortion rates anywhere from 1.4 to 3.4 abortions per thousand women of childbearing age. However, a closer look at datasets and methodologies used in each of the various studies might allow for a more precise estimate of the impact of Medicaid funding limits on state abortion rates.
For instance, the Blank, George, and London study (1996) predicts that public funding limits reduce abortion rates by as much as 3.4 abortions per thousand women of childbearing age. However, this study includes abortion data from the mid-1970s when abortion rates were lower and the data was perhaps less accurate. Hence, the findings appear to be outliers. In my 2014 State Politics and Policy Quarterly study, I ran a series of regressions using abortion data from the Centers for Disease Control (CDC). CDC data on the incidence of abortion tends to be less reliable than data from the Guttmacher Institute. Therefore, these findings can also be excluded as a statistical outlier.
Four of the five remaining analyses find that public finding restrictions reduce abortion rates from 1.44 to 1.63 abortions per thousand women of childbearing age. The findings from my 2014 State Politics and Policy Quarterly study using abortion rate data from the Guttmacher also appear to be something of a statistical outlier. Now, my 2014 study is a stronger study methodologically than my 2011 study. It includes a better dataset of state-level informed consent laws. It also correctly categorizes Illinois as a state that does not publicly fund abortion. That said, since it predicts a significantly larger abortion rate decline than the other four studies, it is probably best to exclude it as an outlier. The remaining studies are fairly consistent in their predictions of how Medicaid funding restrictions impact abortion rates. If we average the results of the four remaining studies, we can predict that Medicaid funding restrictions lower the abortion rate by 1.52 abortions per thousand women of childbearing age. This will allow us to calculate how many lives the Hyde Amendment has saved since 1976.
Methodology
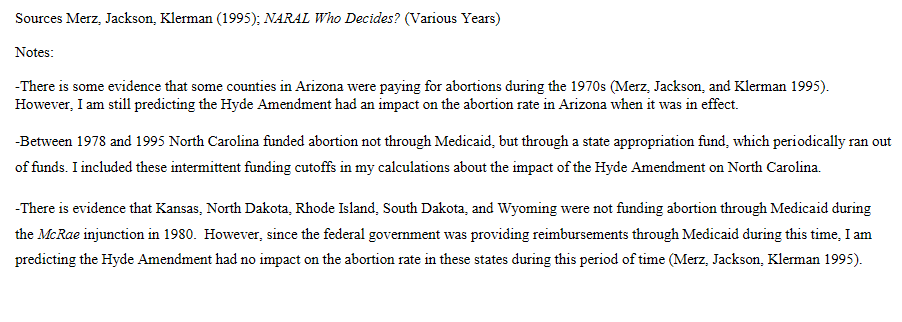
Even though the Hyde Amendment was first passed in 1976, the federal government continued to fund abortions for much of the rest of the 1970s because of legal challenges to the Amendment. Furthermore, even after the Hyde Amendment was upheld in Harris v. McRae in 1980, many states continued to fund abortion through their own state Medicaid programs. Tables 3 and 4 provide detailed information about the years for which the federal government and states were funding abortion through their respective Medicaid programs.

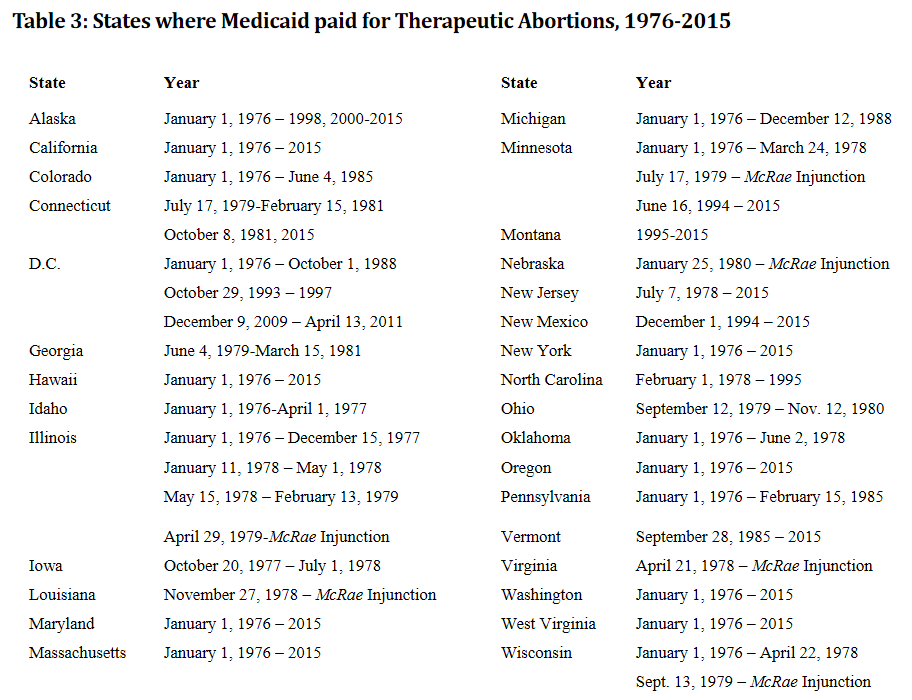
In order to determine the overall impact of the Hyde Amendment we will consider data from all 50 states plus the District of Columbia for every year from 1976 to 2015. The methodology will be as follows:
1) If either the federal government or a state government was funding abortion for Medicaid recipients for the entire year, we predict that the Hyde Amendment would have no impact on the abortion rate.
2) If neither the federal government nor the state government was funding abortion for Medicaid recipients for the entire year, we predict the Hyde Amendment would lower the state abortion rate by 1.52 abortions per thousand women of childbearing age.
3) If neither the federal government nor the state government was funding abortion for Medicaid recipients for part of the year, we predict the Hyde Amendment would lower the state abortion rate by 1.52 abortions per thousand women of childbearing age multiplied by the percentage of the year where abortion was unfunded.
The following examples will further illustrate how the overall impact of the Hyde Amendment will be calculated.
Scenario 1: In 1976, the Hyde Amendment was not in effect due to legal challenges, there-fore it saved no lives in any state in 1976. Similarly, in California in 2015, the state was funding abortions through the state Medicaid program. Therefore, the Hyde Amendment saved no lives in California in 2015.
Scenario 2: In Texas in 2015, neither the state nor the federal government was fund-ing abortions through Medicaid. According to the U.S. Census, there were 5,748,631 women of childbearing age living in Texas in 2015. As such, we predict the Hyde Amendment saved (1.52/1000)*(5,748,631) = 8,738 lives in Texas in 2015.
Scenario 3: In Pennsylvania an injunction on a law limiting Medicaid funding for abortions was lifted on February 15, 1985. As such, Medicaid funding for abortions was limited for 87.4 per-cent of the year (319 days/365 days). According to the U.S. Census, there were 2,690,543 women of childbearing age living in Pennsylvania in 1985. As such, we predict the Hyde Amendment saved (1.52/1000)*(2,690,543)(.874) = 3,574 lives in Pennsylvania in 1985.
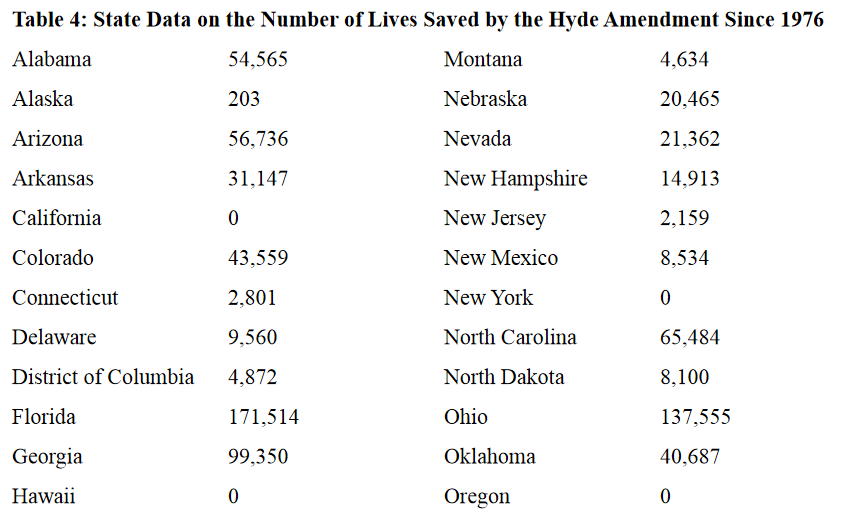
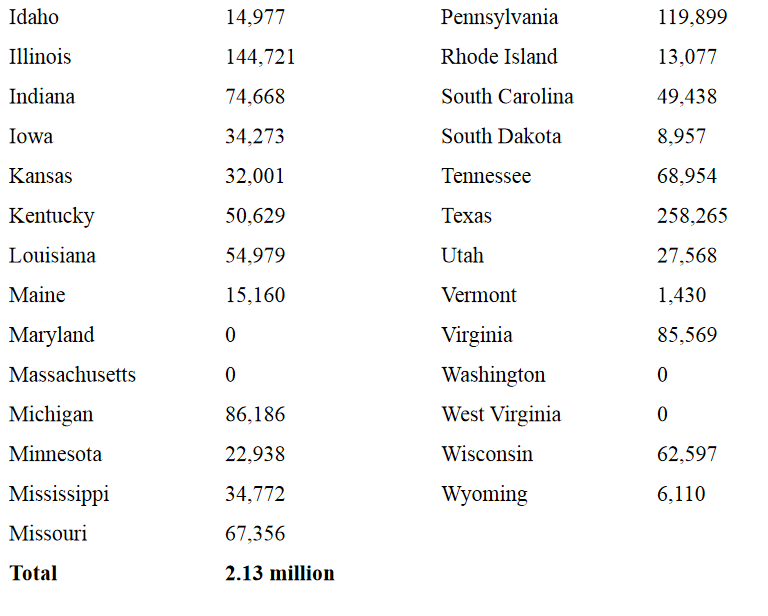
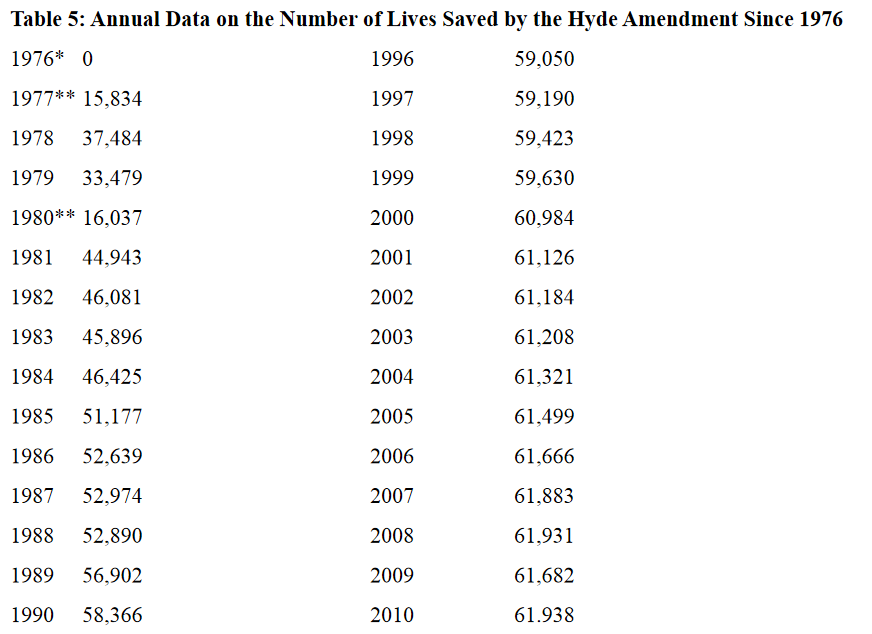
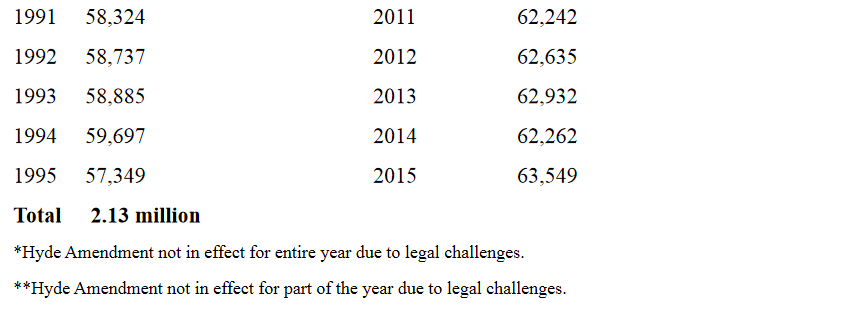
Using this methodology for every state for every year from 1976 to 2016 we predict that the Hyde Amendment routinely saves over 60,000 lives a year and thus cumulatively has saved 2.13 million lives since 1976. Table 4 lists how many lives the Hyde Amendment has saved in each state. Table 5 lists how many lives the Hyde Amendment has saved in each year since 1976.
Conclusion
Ever since the U.S. Supreme Court upheld the constitutionality of the Hyde Amendment in 1980, the abortion rate in the United States has fallen almost every year. The Hyde Amendment is not the only reason for this consistent decline in the abortion rate. Valid research shows that other pro-life laws, shifts in public opinion, and the fact that a higher percentage of unintended pregnancies are being carried to term in recent years are all playing roles in America’s abortion decline. That said, the substantial body of research which shows that public funding restrictions lead to reductions in the abortion rate demonstrates that the Hyde Amendment has certainly played an important role in the long-term reduction in America’s abortion rate.
The Hyde Amendment has been passed every year since 1976 as a rider to the federal Labor/Health and Human Services Appropriations Bill. It has typically enjoyed strong bipartisan support and has been signed into law by both Democratic and Republican U.S. presidents. Even Bill Clinton and Barack Obama, who publicly supported legal abortion, signed the Hyde Amendment into law during their respective presidential administrations. In recent years, however, the Democratic Party has become increasingly supportive of legal abortion and hostile to the Hyde Amendment. In fact, this summer for the first time ever, the Democratic Party’s presidential platform explicitly calls for the Hyde Amendment’s repeal (Richardson 2016).
Numerous polls and surveys show that majorities of Americans continue to oppose having their tax dollars used to pay for abortion. A Marist/Knights of Columbus poll that was released this past January found that 69 percent of Americans oppose taxpayer funding of abortion. Additionally, even 51 percent of people who identify as “pro-choice” oppose public funding of abortion (Knights of Columbus 2016). More importantly, this analysis shows that the Hyde Amendment is one of the most effective tools our nation has to protect the unborn. During the past 40 years, it has saved literally millions of lives. It merits continued support.
Michael J. New, Ph.D. is an associate scholar for the Charlotte Lozier Institute.













