This is Issue 16 of the American Reports Series.
Accurate abortion reporting serves several crucial public health purposes.[1] Complete, precise data enables an accurate estimation of all pregnancy outcomes in the United States as well as the measurement and prevention of unintended pregnancy. It also allows for the evaluation of the impact of laws regulating abortion, both those limiting and those expanding it, as well as other societal factors affecting abortion rates (for instance, the COVID-19 pandemic). However, despite the value of accurate information on abortion, the United States has taken a lax approach to collecting abortion data. Abortion data collection is implemented and maintained by the states, some of which choose not to collect data on abortion procedures. Those that do can voluntarily share their data with the U.S. Centers for Disease Control and Prevention (CDC) to be included in national reports, but because the CDC receives only aggregate data, the information in the national reports is limited. Additionally, the CDC reports are issued on a delayed timetable, with the report for 2018 not expected until late 2021, rendering the report of limited value in assessing current trends.*
To allow for a preliminary view of the current state of abortion in the U.S., the Charlotte Lozier Institute (CLI) reviewed all available state reports for 2017 and 2018. As of July 2020, 38 states had released 2018 abortion statistics. CLI’s preliminary review of 2017 state abortion reporting, published in May 2019, suggested that the long-term decline in abortions in the United States may be slowing.[2] This preliminary review of 2018 state data indicates that the decline may have been interrupted.
Change in Abortions 2017-2018
As of August 2020, 38 states had released reports for 2018. Among these 38 states, total abortions increased by two percent between 2017 and 2018. Twenty-three states individually reported abortion increases, while 15 states reported that abortions declined. The increase in abortions was concentrated in states that tend to be permissive of abortion. In the 13 permissive states, abortions increased by over four percent, while in the 25 states that tend to be protective of life, abortions increased by less than one percent.[3] Among the protective states, there were a little over 2,100 more abortions in 2018 than in 2017. In contrast, in the permissive states, there were almost 5,400 more abortions in 2018.
Protective states were overrepresented in the group of states that published abortion statistics for 2018. Of the 12 states and the District of Columbia that have not released 2018 reports, 11 reporting areas are permissive, compared to just two that are protective. Three permissive states (California, Maryland, and New Hampshire) do not collect any data from abortion providers, and these three states account for approximately a fifth of all abortions occurring in the United States.[4] Additionally, the 13 permissive states included in this report tend to underreport abortions; the Guttmacher Institute’s estimate of the abortions performed in these permissive states in 2017 was 12 percent higher than the abortions actually reported by the states. Guttmacher’s estimate was less than four percent higher than the abortions reported by the protective states included in this report, excluding Georgia, which reports only abortions performed on state residents. Consequently, the change in abortion between 2017 and 2018 may be larger or smaller than available reports reflect.
Five states – Florida, Georgia, Illinois, Nevada, and Virginia[5] – reported increases of more than a 1,000 abortions between 2017 and 2018, although the reasons for these increases vary from state to state. Illinois and Virginia have become more permissive of abortion in recent years, with both states ultimately removing many of their pro-life protections in 2019, and in 2018, Illinois began funding elective abortions for Medicaid-eligible women, leading to an increase in publicly-funded abortions.[6] Florida has reported a rapid increase in chemical abortions. Georgia and Nevada both report fluctuating abortion totals; Georgia’s numbers may be particularly influenced by regional variations, as CDC data shows many women traveling to Georgia for abortions and many Georgia residents going out-of-state.[7] Because Georgia reports abortions performed on residents only, the actual number of abortions occurring in Georgia is higher than the reported totals. Some additional states showed large percentage increases, but due to the relatively low volume of abortions occurring in these states, the actual increase in abortions was small.
Table 1. Change in total abortions between 2017 and 2018 (38 states)
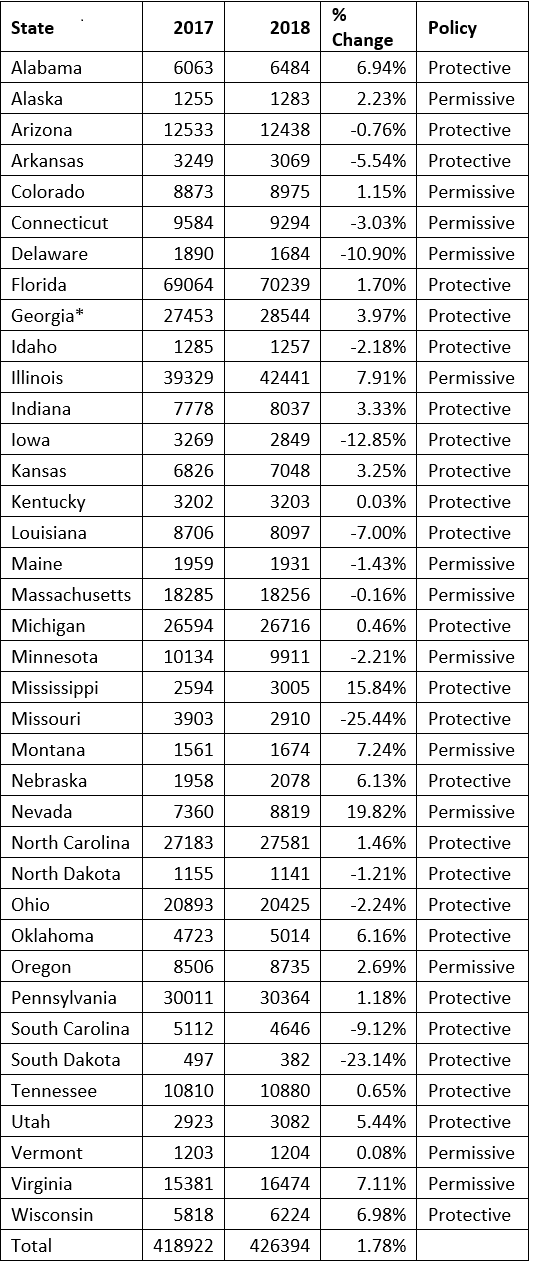
*Georgia only reports abortions performed on state residents.
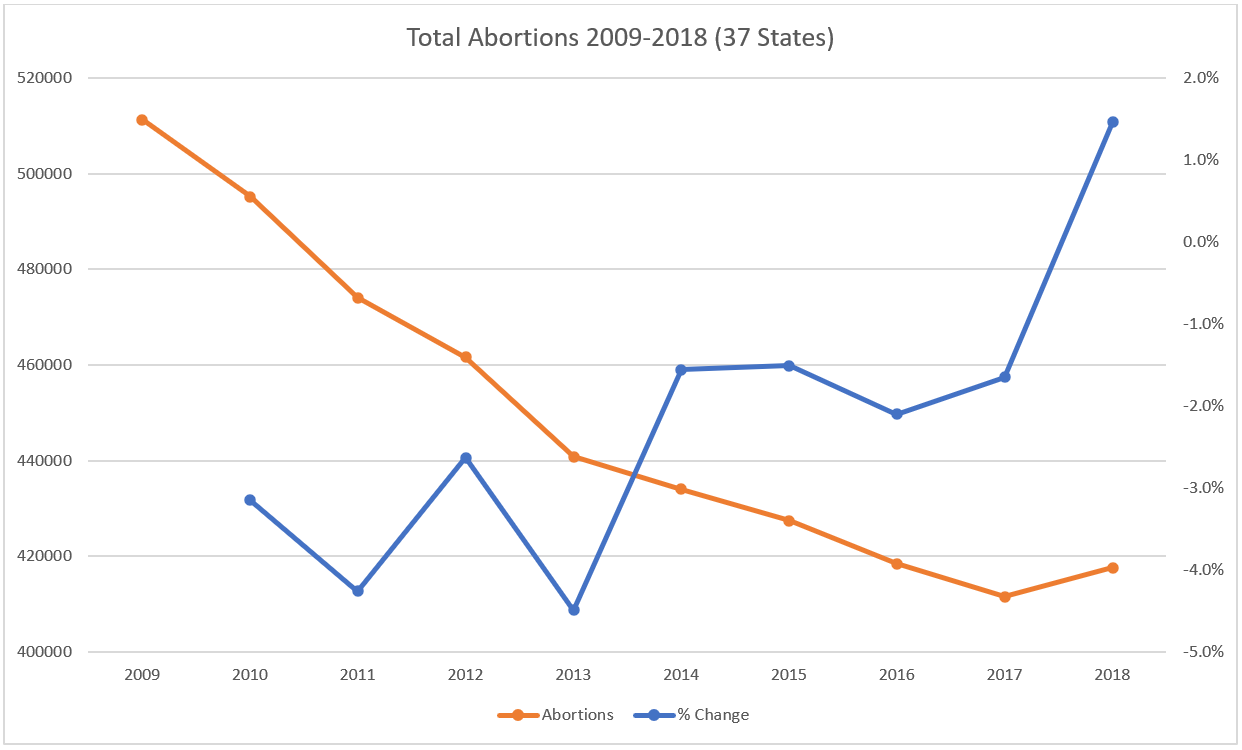
Abortion Trends Over the Past Decade
Thirty-seven of the 38 states had reported consistently over the past decade. Total abortions reported by the 37 states demonstrated a consistent decline in recent years, with abortions falling by 18 percent between 2009 and 2018. While a decrease in overall fertility over this period no doubt contributed to the drop in abortions, it could not account for all the decline: the abortion ratio among the 37 states dropped by 12 percent between 2009 and 2018. Abortion made up a smaller percentage of total pregnancies in 2018 than in 2009, consistent with the downward trend over the past few decades in both the unintended pregnancy rate and the percentage of unintended pregnancies ending in abortion.[8] Still, there was a break in the abortion decline in 2017, with abortions increasing by almost two percent between 2017 and 2018.
The permissive group of states saw a large drop in both the abortion rate (abortions per 1,000 women of childbearing age) and ratio (abortions per 1,000 live births) between 2009 and 2018. Over the 10-year period, the abortion ratio dropped by 14 percent, and the abortion rate fell by 24 percent. The rate and ratio declined by slightly smaller margins among the protective states, with the ratio dropping 10 percent and the rate decreasing 18 percent. However, among the 38 states that reported in 2018, the rate and ratio were far lower in the protective states than in the permissive states. The protective state abortion rate was 10.1, 17 percent lower than the permissive rate of 12.1, and the protective abortion ratio was 167.0, 22 percent lower than the permissive ratio of 215.4. Had the protective states experienced the permissive state abortion rate in 2018, an additional 50,000 to 60,000 abortions could have occurred, making no adjustments for age or race.
Nevada did not report consistently for all 10 years.
Chemical Abortion
Some of the increase in abortions between 2017 and 2018 is attributable to chemical abortion. Thirty-three states reported the number of chemical abortions occurring in 2018. In these 33 states, chemical abortions increased by nine percent from the previous year, while surgical abortions and those performed using other methods dropped by three percent. Previously, CLI estimated that chemical abortions composed 39 percent of all abortions in 2017. CLI estimates that chemical abortions made up 41 percent of the total in 2018. Twenty-nine states reported chemical abortions for every year from 2014 to 2018, and among these states, chemical abortions increased by 42 percent over the five-year period.
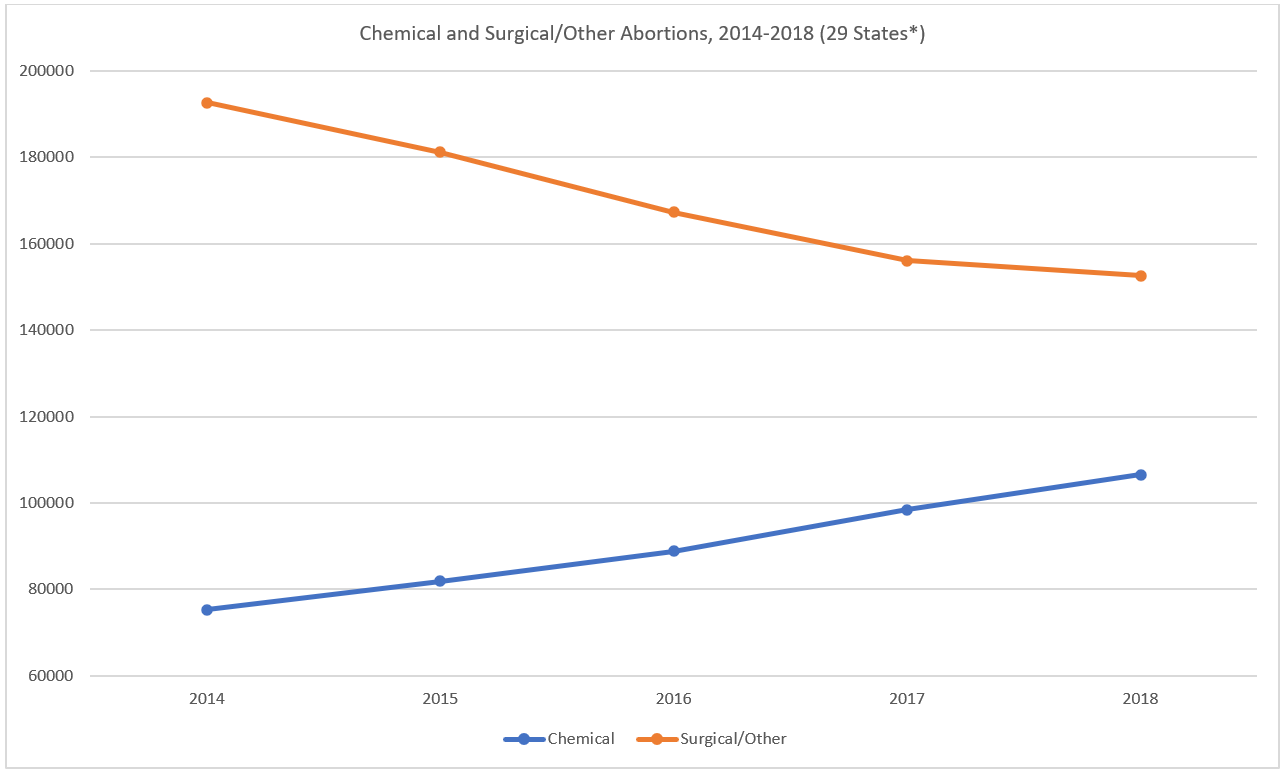
*Of the 29 states, four (AZ, NC, UT, and WI) report only chemical abortions performed on residents
Chemical abortions have been increasing since mifepristone was first approved in 2000 by the U.S. Food and Drug Administration (FDA), a trajectory impacted by several factors, including changing abortion protocols, a fluctuating legal environment, and a shifting abortion landscape in the United States. The abortion industry as a whole has reoriented around chemical abortion. The number of abortion centers in the U.S. has been declining, and some reports indicate that the closures have disproportionately impacted independent centers, rather than large, well-funded abortion chains such as Planned Parenthood.[9] Independent abortion centers are more likely to perform both chemical and surgical abortions, while Planned Parenthood operates many centers that perform chemical abortions only. According to CLI’s last count of Planned Parenthood centers nationwide, just 44 percent of Planned Parenthood abortion centers perform surgical abortions.
Additionally, changing clinical practice may have served to expand the use of chemical abortion. Because mifepristone is a dangerous drug, the FDA maintains a Risk Evaluation and Mitigation Strategy (REMS) requiring abortion providers to distribute the pill from their facilities, rather than from pharmacies.[10] The initial FDA label for mifepristone approved use through 49 days of gestation.[11] However, off-label regimens that prescribed a lower, less-expensive dosage of mifepristone, required fewer trips to the abortion center, and allowed for chemical abortions up to 70 days of gestation were widely used.[12], [13] The National Abortion Federation (NAF), which regularly publishes practice standards for abortion providers, encouraged members to deviate from the FDA-approved regimen,[14], [15] and the experience of states with laws requiring abortion doctors to follow the FDA protocol suggests that the off-label methods led to increased chemical abortion rates.[16] In 2016, the FDA updated the mifepristone label and REMS to reflect these commonly used off-label regimens, but the abortion industry has since further revised the way chemical abortions are performed. The NAF’s clinical practice guidelines for chemical abortion now include recommendations for chemical abortions up to 77 days of gestation and have added the option that women may take mifepristone at home rather than ingesting it at the abortion center;[17] many Planned Parenthood centers now offer chemical abortion through 11 weeks.[18] The NAF also recommends the use of mifepristone for second-trimester induction abortions.
Advances in telemedicine have also contributed to the expansion of chemical abortion. In 2008, Planned Parenthood began performing some chemical abortions via telemedicine.[19] Since then, telemedicine abortion has become widespread in the states that permit it. Usually, a woman undergoing an abortion via telemedicine must still pick up her pills from the abortion center, but the abortion industry has trials underway to allow women to obtain mifepristone from pharmacies or through the mail, despite the fact that this abortion model is currently prohibited by the REMS.[20] A recent court order has suspended the core of the REMS for the duration of the COVID-19 pandemic and may be extended even after the pandemic is over.[21]
However, despite assurances from the abortion industry that these new chemical abortion protocols are safe, there is no comprehensive abortion complication data collection and little oversight. Chemical abortions are known to be riskier and less effective with advancing gestational age.[22] As women undergo chemical abortions later in pregnancy and with less medical care, chemical abortion complications are likely to increase.
Conclusion
This initial review of available state abortion statistics suggests that abortions in the United States increased from 2017 to 2018 and that chemical abortion has played a role in interrupting the long-term decline in abortion rates. As more states release reports, however, these abortion totals could change. In addition, the lack of complete reporting from large, high-abortion-volume states like California means that final 2018 statistics will be missing a sizeable percentage of all abortions occurring in the United States. Without timely, comprehensive abortion reporting from every state, our understanding of U.S. abortion trends will remain incomplete.
*Note: the 2018 abortion surveillance report was published in place of the 2017 report in November 2020. The 2017 tables were published as a supplementary file.
[1] Jatlaoui TC, Eckhaus L, Mandel MG, et al. Abortion Surveillance — United States, 2016. MMWR Surveill Summ 2019;68(No. SS-11):1–41. doi: http://dx.doi.org/10.15585/mmwr.ss6811a1
[2] Longbons T. Abortion in the United States 2017: Preliminary review and a call for reform. Charlotte Lozier Institute. American Reports Series Issue 14, May 2019. https://lozierinstitute.org/abortion-in-the-united-states-2017-preliminary-review-and-a-call-for-reform/ Accessed June 24, 2020.
[3] These groupings were determined by the abortion legislation in place in each state in 2018, the states’ political environments, and the overall trend of their policies. All protective states except for Iowa scored in the top 25 of Americans United for Life’s Defending Life 2018 report, and all permissive states except for Virginia scored in the lower 25. Iowa and Virginia were categorized based on their political environments and the shift in their policies that has taken place over the past decade. See: Americans United for Life. Defending Life 2018. Arlington, VA: Americans United for Life, 2018.
[4] Jones RK, Witwer E, Jerman J. Abortion Incidence and Service Availability in the United States, 2017. New York: Guttmacher Institute, 2019, https://www.guttmacher.org/report/abortion-incidence-service-availability-us-2017. https://doi.org/10.1363/2019.30760
[5] Virginia publishes abortion data in three separate reports. The full report for 2018 has not yet been published and CLI has not posted a 2018 summary.
[6] Longbons T. Abortion reporting: Illinois (2018). Charlotte Lozier Institute. https://lozierinstitute.org/abortion-reporting-illinois-2018/ Published March 6, 2020. Accessed September 17, 2020.
[7] See CDCs Abortion Surveillance System FAQs, “Are Data Available for My Own Analysis?” https://www.cdc.gov/reproductivehealth/data_stats/abortion.htm
[8] See Henshaw SK. Unintended pregnancy in the United States. Fam Plann Perspect. 1998;30(1):24–29 & 46 and Finer LB, Zolna MR. Declines in unintended pregnancy in the United States, 2008-2011. N Engl J Med. 2016;374:843-852.
[9]Abortion Care Network. 2019 Report: Communities Need Clinics. https://www.abortioncarenetwork.org/wp-content/uploads/2019/12/CommunitiesNeedClinics2019.pdf Accessed June 24, 2020.
[10] U.S. Food and Drug Administration. Risk evaluation and mitigation strategy (REMS) single shared system for mifepristone 200mg. https://www.accessdata.fda.gov/drugsatfda_docs/rems/Mifepristone_2019_04_11_REMS_Full.pdf Published April 2019. Accessed June 24, 2020.
[11] U.S. Food and Drug Administration. Drug approval package: Mifeprex (mifepristone) tablet. https://www.accessdata.fda.gov/drugsatfda_docs/nda/2000/20687_mifepristone.cfm Published June 18, 2001. Accessed June 25, 2020.
[12] Jones RK, Boonstra HD. The public health implications of the FDA update to the medication abortion label. Guttmacher. https://www.guttmacher.org/article/2016/06/public-health-implications-fda-update-medication-abortion-label Published June 30, 2016. Accessed June 24, 2020.
[13] Boonstra HD. Medication abortion restrictions burden women and providers – and threaten U.S. trend toward very early abortion. Guttmacher Policy Review. March 2013;16(1). https://www.guttmacher.org/gpr/2013/03/medication-abortion-restrictions-burden-women-and-providers-and-threaten-us-trend-toward Accessed June 25, 2020.
[14] National Abortion Federation. 2015 Clinical Policy Guidelines. Washington, DC: National Abortion Federation, 2015. https://prochoice.org/wp-content/uploads/2015_NAF_CPGs.pdf#page=22
[15] National Abortion Federation. NAF protocol for mifepristone/misoprostol in early abortion in the U.S. https://prochoice.org/wp-content/uploads/Mifeprotocol2013.pdf Revised March 2013. Accessed June 24, 2020.
[16] See: Longbons T. Abortion reporting: Ohio (2017). Charlotte Lozier Institute. https://lozierinstitute.org/abortion-reporting-ohio-2017/ Published December 3, 2018. Accessed June 25, 2020.
[17] National Abortion Federation. 2020 Clinical Policy Guidelines for Abortion Care. Washington, DC: National Abortion Federation, 2020. https://prochoice.org/wp-content/uploads/2020_cpgs_final.pdf#page=22
[18] See https://www.plannedparenthood.org/learn/abortion/the-abortion-pill
[19] Donovan MK. Improving access to abortion via telehealth. Guttmacher Policy Review. 2019;1. https://www.guttmacher.org/gpr/2019/05/improving-access-abortion-telehealth# Accessed September 18, 2020
[20] About the project. TelAbortion. https://telabortion.org/about Accessed June 24, 2020
[21] American College of Obstetricians and Gynecologists v United States Food and Drug Administration. Civil Action No. TDC-20-1320. https://www.courthousenews.com/wp-content/uploads/2020/07/093111166803.pdf Accessed July 27, 2020.
[22] Carlsson I, Breding K, Larsson P-G. Complications related to induced abortion: a combined retrospective and longitudinal follow-up study. BMC Women’s Health. 2018;18(1):158. doi: 10.1186/s12905-018-0645-6.