










What Should We Expect in Maternal Mortality Trends Due to the Dobbs Decision?


This is Issue 11 of the On Women’s Health Series.
Executive Summary
- Dire predictions that abortion limitations would worsen the abysmal U.S. maternal mortality rates pre-date Dobbs, including fearmongering that “TRAP laws” intended to improve the safety and informed consent process of abortion would cause harm.
- These ideologically driven discussions have sidelined important factors such as significant data deficiencies, overrepresentation of minority women in both obtaining abortions and suffering from maternal mortality, and high proportions of unwanted abortions.
- The reckless promotion by abortion advocates of medically unsupervised self-managed drug-induced abortions in pro-life states is likely to cause more harm than the limitations themselves.
- Simplistic comparisons of maternal mortality rates in abortion-restricted states versus abortion-access states ignore the many risk factors for maternal mortality independent of abortion that differentiate these states, such as poverty, chronic illnesses, proportion of childbirth in ethnic minorities, mental health or substance abuse disorders, and access to quality health care.
- Predictions of mass exoduses by healthcare providers from pro-life states have not been realized, nor has evidence of worsening maternal mortality caused by pro-life laws, all of which allow abortion in an obstetric emergency to protect a mother’s life.
Following the U.S. Supreme Court’s 2022 decision in Dobbs v. Jackson Women’s Health Organization, which overturned Roe v. Wade and returned the opportunity to regulate abortion to legislatures, a consistent and compelling allegation has emerged that maternal mortality will increase due to abortion limitations. This has predictably caused many kind-hearted Americans who might otherwise support pro-life laws to turn against them due to fear the laws would harm women in crisis. Many are aware that the U.S. maternal mortality rate has been among the highest in the developed world for decades,[1] and fear any policy changes that would increase a woman’s risk of this devastating event.
Even prior to the court’s monumental decision in Dobbs, abortion advocates began advancing this prediction in anticipation that Roe would eventually be overturned. A 2021 article (published after Texas began enforcing its Heartbeat Law[2]) written by a pro-choice abortion researcher—“The Pregnancy Related Mortality Impact of a Total Abortion Ban in the United States: A Research Note on Increased Deaths Due to Remaining Pregnancy”[3] —predicted “that in the first year of a total abortion ban, estimated pregnancy-related deaths would increase from 675 to 724 (49 additional deaths, 7% increase), and in subsequent years to 815 (140 additional deaths, 21% increase).” These predictions were made based on uncritically accepting the Centers for Disease Control and Prevention’s (CDC’s) National Vital Statistics System (NVSS) maternal mortality data for childbirth compared to abortion in 2017 and estimating that each abortion denied would result in 0.8 additional births, with the attendant risk of additional deaths if the number of women who obtained abortions at that time instead carried their pregnancies to term.
Before proceeding further, it is important for the reader to be aware that there are several disparate maternal mortality reporting systems in the U.S. using different methods of data analysis and different temporal definitions, each with pros and cons, as we have previously discussed.[4]
When a woman’s death is identified during pregnancy or within one year of the end of the pregnancy, regardless of the cause, it is called a “pregnancy-associated death.” If analysis determines the cause was related to or aggravated by the pregnancy or its management, it is subcategorized as a “pregnancy-related death.” The CDC’s NVSS determines pregnancy-related deaths based on death certificate International Classification of Diseases, Tenth Revision (ICD-10) coding during or within six weeks of a pregnancy. This method assumes the accuracy of death certificate coding, which is sometimes in error, but it allows rapid documentation of U.S. maternal mortality rates for comparison to other countries.
The CDC’s Pregnancy Mortality Surveillance System (PMSS) determines pregnancy-related deaths based on death certificate documentation of pregnancy within one year and an in-depth review of the woman’s medical records by CDC epidemiologists. Additionally, state Maternal Mortality and Morbidity Review Committees (MMMRCs) comprehensively review reported maternal deaths through medical records, police reports, and informant interviews. Although these multidisciplinary committees ultimately provide better quality data, the analysis is time-consuming. As an example, the Texas MMMRC has only recently completed analysis of the years 2021 and 2024, but has yet to begin analysis of the years 2022 and 2023.[5]
This pro-choice author predicted that “Black woman would experience the greatest increase in deaths” (with a 12% increase in the first year and a 33% increase in subsequent years), followed by Hispanic women (with a 6% increase in the first year and an 18% increase in subsequent years).[6] It is tragic that the Black population has been overrepresented in both maternal mortality and abortion statistics for decades (with approximately three times the rate of maternal mortality as well as three times the rate of abortions),[7] so it is not surprising they would appear to be disproportionately affected by a theoretical abortion ban. Subsequent to this rationale, abortion has been promoted to Black women with the fatalistic narrative that the healthcare system cannot adequately protect them from death in childbirth without ridding them of their unborn children.[8] Sometimes this recommendation is prefaced with the allegation, as in this article, that “structural racism is a fundamental cause of maternal health inequality.” In other words, it is implied that racism within the health care system is to blame for Black women’s deaths, sometimes failing to consider other contributing factors.[9]
Unfortunately, this narrative may worsen the problem, as encouraging suspicion of the health care system among Black women may cause them to fail to seek necessary medical care in a timely fashion, potentially causing anticipated bad outcomes to become a self-fulfilling prophecy. Nonetheless, a dispassionate observer should immediately recognize the cynical utilitarian ideology that promotes one human’s death in an attempt to prevent another human’s death. Surely, our society can do better than that. We must work harder to find the true causes and solutions.
This author ignores or is unaware of the substantial data deficiencies affecting the collection of maternal mortality data, particularly abortion-related mortality data.[10] We have addressed these deficiencies in detail elsewhere,[11] but in brief, there appears to be substantial undercounting of deaths following abortion,[12] particularly “deaths of despair” resulting from mental health causes such as suicide, intimate partner homicide, substance abuse and overdose, and accidental deaths from high-risk-taking behavior.[13] International studies indicate a woman is up to six times as likely to die from suicide in the year following abortion compared to childbirth, and at least twice as likely to die from any cause.[14] Thus, the assumption that abortion will protect a woman from death by preventing the completion of her pregnancy with the possible attendant risks of severe complications of childbirth, is unwarranted. Whether a woman dies from mental health complications or pregnancy related complications, she still leaves a mourning family and community, and her death creates an impact. This argument also pessimistically ignores the value of the new living human being who enters the world through childbirth, with his or her immeasurable worth and value.
This author also assumes that unintended pregnancy rates would stay constant if abortion were limited, causing abortion rates in the absence of restrictions to stay the same each year. This ignores the likelihood that couples would make behavioral changes if abortion were not readily available. Perhaps they would use more effective contraception such as long-acting reversible contraceptives (copper and levonorgestrel intrauterine devices or Nexplanon implant) or obtain permanent sterilization (bilateral tubal ligation or vasectomy), which all have failure rates less than 1%, as compared to failures as high as one in five women yearly when barrier methods are used.[15] Additionally, couples may decrease promiscuous behavior, decreasing the likelihood of unintentional pregnancies at risk for abortion. Real-world studies show that in the presence of abortion limitations, the unintended pregnancy rate decreases with time.[16]
The assumption is also made that all abortions are desired by the women who obtain them, but in fact, one survey demonstrates 60% of women with a history of abortion would have preferred to give birth, and would have done so if they had access to more material, financial, or relationship resources.[17] Even a study by pro-abortion researchers documented that almost all women who encounter barriers to abortion subsequently grow to desire their child and retrospectively state they are glad they gave birth.[18] We should all recognize the tragedy of unborn life lost through abortion when women would prefer to give birth or would quickly reconcile themselves to having a child.
The Stevenson article on the “pregnancy-related mortality impact of a total abortion ban” also notes that “[m]uch attention has focused on anticipated increases in potentially unsafe abortion outside the clinical context and resulting pregnancy-related deaths.” The author further opines that “inference from historical evidence is of limited salience because pregnancy-related mortality before Roe v. Wade legalized abortion nationwide was largely due to unsafe abortion, the prevalence of which would likely be different under a contemporary total ban. This prevalence is particularly difficult to project because of recent advances in safer self-managed medication abortion.”[19] Other abortion advocates have echoed the fearmongering narrative that women will resort to unsafe abortion in the presence of abortion limitations.[20]
There are two important points to emphasize here. The threat that women will self-manage their abortions in unsafe ways has been used as a cudgel to promote legalized abortion since prior to Roe v. Wade, but examination of history demonstrates that 90% of abortions prior to Roe were performed by physicians, in medically standard ways (D&C), albeit illegally. Abortion was becoming safer long before it was widely legalized due to advances in surgical techniques, safer anesthesia, and widespread antibiotic use. The commonly cited statistic of 5,000 to 10,000 women dying yearly from unsafe abortions was an invention of abortion advocates, when in fact, the CDC documented fewer than 100 deaths yearly from both legal and illegal abortions prior to Roe.[21]
In fact, analysis of the years surrounding the Roe v. Wade decision demonstrates that the overall maternal mortality rate was steadily improving before readily accessible abortion was available. From 1964-1966 maternal mortality in the U.S. was 31.4/100,000 live births. From 1970-1972 it dropped to 19.8/100,000 and declined still further after Roe to 14.2/100,000 from 1973-1975. Prior to Roe in 1972, the 29 states that had restrictive abortion laws had a maternal mortality rate of 19.3/100,000, which compared favorably with the 16 states with permissive laws that had a maternal mortality rate of 20/100,000.[22]
Conversely, however, de-medicalized provision of abortion drugs through on-line ordering and mail distribution has been increasingly promoted under the cover of “access” and “autonomy.”[23] The “recent advances in self-managed medication abortion” referenced by Stevenson in her 2021 article[24] have caused the procedure to become much more dangerous.[25] The fault of this does not lie with abortion limitations, but with the insistence of the abortion industry to promote medication abortion in increasingly dangerous ways.[26] Unfortunately, however, when these unsafe abortion techniques do result in complications, they may remain unrecognized because women are often advised not to disclose the information.[27] Abortion advocates will then blame the complications on pro-life laws rather than the reckless endangerment of women caused by abortion advocates themselves.[28]
Prior to the Dobbs decision, attempts were made to connect discrete and limited abortion legislation, so called “Targeted Regulation of Abortion Providers” or “TRAP” laws, to higher maternal mortality in pro-life states. For example, in 2022 the Commonwealth Fund published, “The U.S. Maternal Health Divide: The Limited Maternal Health Services and Worse Outcomes of States Proposing New Abortion Restrictions.”[29] Here they argued that states with restrictions cumulatively had maternal death rates 62% higher than those without restrictions (28.8 vs. 17.8/100,000 live births in 2020). Their topline summary stated, “In states that have banned or restricted abortion access, rates of maternal and infant deaths are much higher than in states that have preserved access” and, then, concluded “Making abortion illegal makes pregnancy and childbirth more dangerous; it also threatens the health and lives of all women of reproductive age.” For the lazy reader, or uncritical journalist reporting on this article, the conclusion seems clear and there appears no need to actually read the article to understand its nuances.
But what constitutes a TRAP law? In the 1992 Supreme Court decision, Planned Parenthood v. Casey, the court introduced an “undue burden standard” whereby an abortion law was considered unconstitutional if it placed “a substantial obstacle in the path of a woman seeking an abortion before the fetus attains viability.”[30] Thus, gestational age restrictions were often struck down, but many TRAP laws were allowed to stand. Broadly, TRAP laws aim to improve informed consent or safety for a woman considering abortion, with limits such as mandatory waiting periods, pre-abortion ultrasound, parental consent requirements, and provider or facility standards. Again, a closer look is warranted to determine how laws such as these would contribute to maternal mortality.
The argument has been made by abortion advocates that TRAP laws limit access to abortion, initiating lawsuits both prior to and subsequent to Dobbs in states that have passed constitutional amendments guaranteeing abortion until the time of viability (generally considered to be around 22-24 weeks of gestational age). But a closer examination of some specific TRAP laws documents they may be necessary to protect a woman inquiring about abortion, both to provide adequate informed consent while she makes her decision and to provide quality medical care before, during and after the abortion.
For example, Planned Parenthood recently sued the state of Missouri, which allows abortion to viability, to overturn any remaining laws addressing abortion practices. A requirement that patients receive state-mandated education containing material with illustrations of fetal development and information about resources available to assist a woman if she desires to give birth to her child was called the “Biased Information Law” by the plaintiffs. They objected to a requirement that a woman meet in-person with the physician who would be performing her abortion 72 hours before the procedure to discuss the details, and to give her a chance to change her mind once she understood the reality of the procedure. They similarly sought to remove requirements for ultrasound and physical examination before the procedure, although these commonly performed medical procedures will convey critical information such as accurate gestational age, presence of intrauterine viable pregnancy, and uterine abnormalities. Failure to recognize in advance women who are not candidates for a particular abortion procedure will increase the risk of complications and failures.[31] They also opposed requirements for facility standards and admitting privileges that ensure an abortionist would be available to care for any complications he might cause in a hygienic environment. They protested against a medication abortion complication plan requirement that would educate a woman on how to obtain emergency care if she should suffer a complication from her medication abortion, particularly if she lived in a rural area far from the abortionist. Other provisions against which they remonstrated included required medical malpractice coverage, pathologic examination of tissue, and complication reporting requirements.[32]
These actions demonstrate the abortion industry desires to operate independent of any medical supervision, apparently prioritizing profits over the safety of the women it professes to care for. It is clear these limitations would improve safety for women seeking abortion and prevent unwanted abortions, so one cannot make a coherent argument that TRAP laws will increase the risk of maternal mortality.
What factors unrelated to abortion may place a woman at risk for maternal mortality? There are many complex factors that may contribute to maternal mortality, such as poverty, chronic illness, limited access to quality health care, and mental health or substance abuse disorders.[33] It is possible these risk factors may be overrepresented in women who live in pro-life states or belong to certain ethnic groups, placing them at higher risk of maternal mortality, independent of their state’s ease of abortion access.
A graphic from the Commonwealth Fund article demonstrates the 26 states they defined as abortion-restrictive are primarily located in the South and Midwest, areas which are overrepresented by poverty,[34] poor healthcare access,[35] minority (especially Black) populations,[36] and have long histories of poor public health outcomes.[37] Conversely, the 24 states (plus the District of Columbia) defined as having ready abortion-access are located primarily in the Northeast and West Coast. Generally, the Northeast and West Coast have higher population densities and more urban-centric economies compared to the South and Midwest, which hold larger rural populations.
A second graphic from the report demonstrates more births in abortion-restrictive states overall, with a concomitantly larger percentage of births to Black mothers (17.3% compared to 11.7% in abortion-access states). An important point should be emphasized here. If more births occur in a population at high risk for maternal mortality (risk which has been demonstrated repeatedly in the Black population), one would anticipate more deaths to occur if the conditions that place these women at risk are not modified. A greater percentage of births to high-risk populations is one obvious reason that abortion-restrictive states might have worse maternal mortality rates. The solution is not to further increase this population’s abortion rate, which has its own set of risks,[38] but to address the true causes of maternal mortality in the population. It is cynical to assume that only by ending the lives of the unborn children of high-risk women will we be able to impact their heart-breaking maternal mortality statistics.
What other factors differentiate the states that have pro-life laws from states that don’t? The article then proceeds to list other factors unrelated to abortion which may contribute to higher maternal mortality. Critically, there are fewer maternity care providers in abortion-restrictive states. They have a 32% lower ratio of obstetricians to births and a 59% lower ratio of certified nurse midwives to births compared to abortion-access states. Additionally, they have more maternity care deserts (39% vs. 25%), and more women giving birth in rural areas (17% vs. 8%), and maternal mortality is documented to be higher when access to quality medical care is limited by medical resources or geography. The restrictive states have higher overall death rates for women of reproductive age, indicating that the population at risk for becoming pregnant may be less healthy at baseline. The authors report there are greater racial inequities across the health care systems of abortion restrictive states, though this is poorly defined. In 2020, in abortion-restrictive states, the proportion of individuals giving birth who had no prenatal care or late prenatal care was 62% greater than for someone giving birth in abortion-access states (7.3% vs. 4.5%). Clearly, barriers to access to quality medical care contributes to the elevated risk for women in abortion-restrictive states.
The article also reported the source of payment was Medicaid in 44.8% of deliveries in abortion-restrictive states vs. 38.7% in abortion-access states, compared to private insurance in 47.3% vs. 54.6%, and self-pay in 4.9% vs. 2.7%, respectively. Since Medicaid insurance provides coverage to people with low incomes or disabilities,[39] this group could be expected to have more pre-existing risk factors for maternal mortality, and thus states that have a higher proportion of population covered by Medicaid might reasonably be expected to have more adverse outcomes.
As the article noted, The American Rescue Plan Act of 2021 gave “states the option of extending Medicaid coverage for up to one year following a Medicaid-financed pregnancy or birth,” thus extending coverage from the 60 days postpartum required by federal law. Many conservative states were hesitant to accept this federal funding initially, and the article reported that less than a third of abortion-restrictive states had adopted this coverage extension, or had plans underway to do so, compared with almost half of abortion-access states (when the article was written in 2022). Pre-pregnancy and post-pregnancy insurance coverage might be expected to allow a woman better healthcare access, presumably improving pre-pregnancy health or providing better treatment for post-pregnancy medical conditions, so it is plausible that states providing better insurance coverage (as the abortion-access states appear to do) would have decreased maternal mortality in the population as a whole.[40] Of note, the CDC PMSS and MMRCs measure maternal mortality until one year postpartum, so an extended duration of insurance coverage for women with chronic illnesses is likely to provide a positive impact.
The report optimistically concludes: “States have it within their power to avoid that outcome. In partnership with health plans, providers, and residents, state leaders could attempt to recruit more maternity care providers—including midwives, physicians, doulas, and nurses—and promote the operation of more birthing facilities, such as hospital units and birthing centers. Additional support could be provided to community-based organizations and to perinatal health care teams…” They also advocated for: “Increased federal funding for reproductive health care, family planning, maternity care, and care delivery system transformations to mitigate the impact of the Dobbs decision and state abortion bans on people’s lives.”[41] Thus, we discover that the Commonwealth Fund report contains a mixed bag of truths and untruths. Although they failed to prove their allegation that abortion limitations have led to the maternal mortality disparities between these states, their policy recommendations (except for proposals to increase abortion access) may provide some relief for the states whose mothers have been hardest hit.
A 2024 ideologically driven report from the Gender Equity Policy Institute (GEPI), “Maternal Mortality in the United States After Abortion Bans,” has been widely covered by pro-abortion media.[42] The report began with several “Key Findings.” These included: “Mothers living in states that banned abortion [were] nearly 2x as likely to die during pregnancy, childbirth, or soon after giving birth, compared to mothers living in supportive states where abortion was legal and accessible. Maternal mortality fell 21% in supportive states post-Dobbs. Maternal mortality rose 56% in Texas in the first full year of the state’s abortion ban; up 95% among White women. Black mothers living in banned states were 3.3x as likely to die as White mothers in those states. Women’s risk of maternal death in Texas was 155% higher than in California. Latina mothers in Texas faced nearly triple the risk of maternal mortality as those in California.” Once again, pro-abortion researchers trumpeted an association between pro-life laws and increased maternal mortality, allowing ideological journalists the opportunity to cease their investigation with the top-line conclusions and promote this narrative, without investigation of what the study really found.[43]
The GEPI document was self-published and not peer-reviewed. While the analysis did show rising maternal mortality rates in Texas in 2020 and 2021 (during the Covid-19 pandemic), it also showed the Texas maternal mortality rate fell by more than 35% in 2022—the year the Texas Heartbeat Act would have been expected to have an impact. The authors also noted that “in each year from 2019 to 2023, maternal mortality was highest in banned states and lowest in supportive states,” demonstrating that high maternal mortality rates predated Dobbs.
The Covid-19 pandemic makes these comparisons difficult, as the authors acknowledged in an appendix. During the pandemic numerous disruptions occurred in the U.S. healthcare system. Many medical offices closed temporarily, and patients were encouraged not to come for routine visits, only emergencies. This may have delayed detection of potentially serious obstetric events such as preeclampsia or fetal growth abnormalities. Some patients feared seeking care from emergency rooms and hospitals, which might also have led to delays for treatment of emergencies. Covid-19 was estimated to contribute to “one quarter of all deaths in 2020 and 2021 combined.” Notably, deaths during the pandemic were most pronounced in women > 40 years old, American Indian women, and Black women. Women with pre-existing health problems, such as obesity, hypertension, diabetes, and other chronic illnesses were disproportionately impacted by Covid-19,[44] so it is difficult to disentangle the effects of the virus from abortion legislation. A cursory examination of CDC NVSS data cannot reliably document whether the declines between 2021 (Covid-19 peak year) and 2022 are related to resolution of the pandemic or abortion limitations or some combination of the two (or even other factors).
The GEPI obtained their data from the CDC’s NVSS, which is the system most prone to error, as it relies solely upon ICD-10 coding on death certificates, with the assumption they are accurate. There are many methods of identifying and examining deaths, as discussed earlier, but notably the most reliable methods depend upon in-depth analysis of women’s medical records and other contributing information, which the CDC NVSS does not do.[45]
Despite a variety of contributing factors discussed within the report, the ideologic bias of the GEPI researchers was demonstrated by Nancy L Cohen, its president, when she confidently stated, “There’s only one explanation for this staggering difference in maternal mortality. All the research points to Texas’ abortion ban as the primary driver of this alarming increase.”[46]
Much of GEPI’s attention focused on Texas, where they reported that from 2019 to 2022, the rate of maternal mortality cases rose by 56%, compared with just 11% nationwide during the same time period. In 2021, with its “Heartbeat Act,” Texas was the first state able to enforce a strict abortion limitation, even prior to the Dobbs decision,[47] and has subsequently been the focus of much scrutiny. Examined by ethnicity, GEPI reported maternal mortality in Hispanic women increased from 14.5 maternal deaths per 100,000 live births in 2019 to 18.9 in 2022; in white women it nearly doubled, rising from 20 per 100,000 to 39.1; and in Black women it rose from 31.6 to 43.6 per 100,000 live births.
Since the GEPI report introduced the comparison between Texas and California, it would be helpful to look deeper at factors unique to and held in common between the two states. They both have large populations (California 39.3 million and Texas 32.1 million[48]) and many births (Texas’ birth rate is 59.3/1,000 reproductive aged women and California’s is 49.8/1,000 reproductive aged women[49]). The number of abortions is difficult to know with certainty, due to lack of federal mandatory reporting and California’s refusal to provide any data to the CDC, but in 2020 (prior to implementation of any gestational age restrictions by Texas), the CDC documents 55,132 abortion occurred in Texas[50] and the Guttmacher Institute reported 154,060 abortions in California,[51] nearly three times as many as Texas. One final note is that although both states have large populations of undocumented immigrants (California with an estimated 2.3 million and Texas with an estimated 2.1 million[52]), California readily provides Medi-Cal (their state Medicaid program) to undocumented pregnant women,[53] whereas Texas does not, and anecdotal reports describe sick women in Texas delaying necessary medical care due to immigration enforcement concerns and lack of insurance.[54] California has a generous welfare state that provides public funding for contraception, abortion, other pregnancy services and a full year of Medicaid coverage postpartum. I am noting this, not to make specific policy recommendations, but to document that far more women in California have health care access than in Texas.
Texas has higher poverty,[55] higher uninsured,[56] a significant undocumented population,[57] higher chronic illness,[58] and more rural maternity care deserts[59] compared to many other states. These factors are often interrelated, but none are related to pro-life laws.[60]
To their credit, physicians and policymakers in California became very serious about addressing the maternal mortality crisis once they recognized its severity, and in an impressive fashion, implemented changes that significantly dropped maternal mortality in four years, from 14 to 6.2/100,000 live births.[61]
Certainly, facilitating the abortions of high-risk women would be expected to reduce maternal mortality by causing fewer high-risk women to undergo the high-risk activity of childbirth; but, again, one must note the cynical nature of promoting the immoral action of abortion to address the heartbreaking problem of maternal mortality. California’s extremely high abortion rates cannot be condoned as a solution.
So, one must ask, what ethical actions has California taken that may have impacted the problem of maternal mortality, and how can states like Texas learn from them?
The first important step was to focus on improving data collection. It has been well documented that the U.S. does not identify all deaths temporally associated with pregnancy due to overreliance upon death certificates which often fail to report an associated pregnancy,[62] causing many maternal deaths to remain unknown and unexamined. California researchers began to link birth certificates with death certificates in reproductive aged women. This markedly increased detection of maternal deaths associated with childbirth that were unknown by death certificates, but the researchers noted that this action could not be performed to detect early pregnancy losses, such as ectopic pregnancies or miscarriages, due to lack of mandatory fetal loss certificates. In order to improve detection of deaths associated with early pregnancy events, the “committees comb(ed) through news clippings or hospital records.” Unfortunately, these methods could not reliably detect abortion-associated deaths because media are often hesitant to report on deaths following abortion, and many abortion-related complications are miscoded in hospital records as being miscarriage-related instead.[63]
Once they had improved detection and analysis of maternal deaths, California discovered women were dying in large numbers from catastrophic events in childbirth such as heart disease, hemorrhage, and hypertension. Researchers at Stanford University, led by Dr. Elliott Main, created the California Maternity Quality Care Collaborative to develop “toolkits,” detailed emergency plans to address pregnancy emergencies, improving the response of doctors and hospital systems. To date, they have developed toolkits addressing cardiovascular disease, community birth transfer (when a higher level of care is needed), elimination of early elective deliveries (with attendant complications of prematurity), hemorrhage, hypertensive disorders, sepsis, substance exposure (drug abuse), supporting vaginal birth (preventing the frequent complications of cesarean deliveries), and venous thromboembolism.[64] Other obstetric organizations, such as the American College of Obstetricians and Gynecologists (ACOG) and the Alliance for Innovation on Maternal Health (AIM) have also noted this need and have created similar safety bundles.[65]
Finally, the state began to create databases that linked hospital discharge data with birth certificates to provide important metrics to inform the public (like making c-section rates available on Yelp).[66] This resulted in hospitals being held responsible for the quality of care they provided, and this transparency ultimately led to a decline in c-section rates, which are associated with higher maternal mortality.
While California has led the way in proactively addressing maternal mortality, Texas is following their lead, albeit belatedly, in many of their evidence-based recommendations. The Texas MMMRC, which also suffered significant data deficiencies, has also begun records-linkage of birth certificates with death certificates in reproductive aged women, with subsequent improved identification of deaths associated with childbirth.[67] Texas has likewise begun to encourage the use of AIM toolkits to improve rapid recognition and response to obstetric emergencies, including recognition of maternal early warning systems in pregnancy (MEWS), obstetric hemorrhage, severe hypertension, venous thromboembolism, maternal sepsis, and cardiac conditions complicating obstetric care.[68] Texas has been criticized for its many uninsured pregnant and postpartum women, but in 2023, the Texas legislature extended Medicaid for Pregnant Women coverage to 12 months after pregnancy instead of the 60 days it had been allowing.[69]
Allegations of provider shortages are intended to foment fear in pro-life states. Dr. Tamika Auguste, an ob/gyn and board chairman of the pro-abortion ACOG Foundation Board, in a 2024 article on maternal mortality stated, “We are setting ourselves up for an absolute reproductive health provider shortage, and contributing to that is this interference into the patient-provider relationship and the restrictions that are being placed on us.” In case it was not clear what interference she referenced, the journalist then began discussing abortion restrictions with the implication that the restrictions themselves were driving out women’s health care providers.[70]
Similarly, the Commonwealth Fund 2022 report worried, “After the Dobbs decision, this (provider) disparity could worsen, as some maternity care providers have been reported to be reluctant to work in states where they might face legal challenges to their practice.”[71] They doubled down in their 2024 report, “Tighter limits and additional bans on abortion are certain to drive more maternal and reproductive health care providers to shut down or leave their states, deepening the crisis of access to maternity care. Abortion bans threaten American’s future access to care across all medical specialties; in fact, since 2022, medical residency applications in states with bans have declined by more than those in other states.”[72]
While these allegations would be compelling if true, there is no evidence that there is a mass migration of ob/gyns or other medical providers out of pro-life states, nor a deficit in doctors willing to train in these states. During the 2023-2024 academic year, medical schools granting M.D. degrees in pro-life states increased enrollment by 6.6-7% compared to 2019-2020 enrollment. States with no abortion limits, conversely, increased enrollment by only 4.6%. Osteopathic medical school enrollment has also increased dramatically in recent years, and over half of osteopathic schools are located in pro-life states. Nearly 87% of applicants for ob/gyn residencies applied to programs in pro-life states,[73] and virtually all residency positions were filled in the 2026 ob/gyn match.[74]
A 2025 study from JAMA Network Open documented there was no net migration of ob/gyns after Dobbs, but in fact, there were increases throughout the country, as the number of ob/gyns increased by 8.3% in states with limitations on all elective abortions, 10.5% in states with lesser abortion limitations, and 7.7% in states where abortion was protected.[75] The reality is the vast majority of ob/gyns do not perform elective abortions,[76] so pro-life laws (as long as the emergency exceptions are properly understood) should not affect their practice or cause them to change locations.
Hospital and Labor and Delivery closures resulting in maternity care deserts are a long-term problem that precedes the Dobbs decision, usually resulting from financial strain brought on at least partially by too few deliveries.[77] So, ultimately more deliveries facilitated by pro-life laws should improve the prospects of facilities providing women’s care.
All pro-life states allow an exception permitting abortion if it is necessary to prevent a mother’s death and often to prevent severe impairment of a major bodily function, so abortion restrictions should not increase risk in obstetric emergencies.[78] None of the laws require that the threat be imminent, nor that a doctor be certain that the complication will cause death, or even that a consensus of physicians exist, allowing a physician to use his “good faith” or “reasonable medical judgment” to make the determination.[79] When an obstetrician diagnoses a complication that can lead to severe illness or death, he does not know for sure if a woman will die, or how quickly her condition may worsen, but he is given deference by pro-life laws to use his clinical judgment to determine if intervention, including abortion, is indicated.
Notwithstanding, ProPublica and other pro-abortion media have highlighted many examples of substandard medical care in pro-life states, implying that delayed or poor-quality care was caused by abortion limitations, rather than placing the blame where it belonged, on individual physicians’ actions or inaction. For example, when two women died in Georgia following complications from mifepristone and misoprostol abortions, and two women died in Texas from inappropriate treatment of miscarriages, and a third died in Texas from sepsis (at a gestational age when her child could have survived delivery), they blamed pro-life laws rather than the doctors’ poor care.[80] Notably, three of the Texas doctors were sanctioned by the Texas Medical Board, demonstrating that indeed their lack of action was not required by the state’s law.[81] Physician fear of prosecution is inappropriate, as no doctor has been prosecuted for performing an abortion to protect the life of the mother in many decades.[82]
What does the preliminary maternal mortality data since Dobbs show? No data exists proving that any state’s abortion laws directly caused a rise in maternal mortality and, in fact, the trends are improving in most pro-life states.
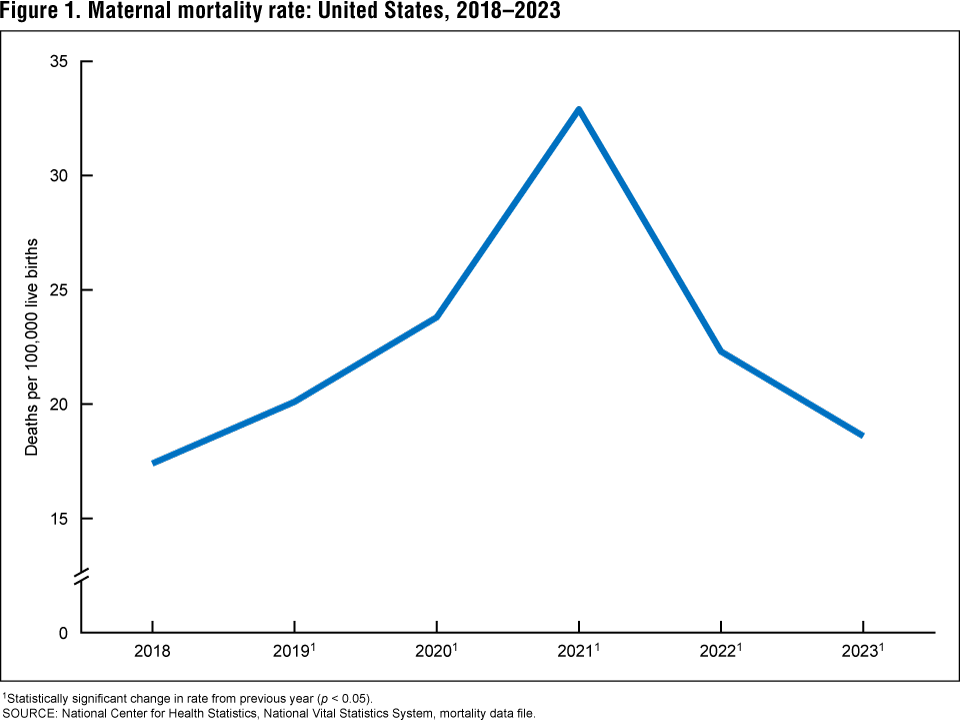
The CDC NVSS documents dramatic improvement in U.S. maternal mortality in recent years, from 32.9/100,000 live births in 2021, to 22.3 in 2022, to 18.6 in 2023, to 17.9/100,000 in 2024.[83] A CDC graph shows that after a high in 2020-2021 (peaked in Feb 2022 at 33.8) related to the Covid pandemic, rates overall have dropped dramatically.[84] Provisional CDC NVSS maternal mortality rates until 2025 demonstrate that overall U.S. MM was lower in December 2025 (16.6) than in January 2019 (17.4).[85]
This data has not yet been broken down by state, but it is encouraging to see that overall, the dire predictions about worsening maternal mortality in the U.S. have not been proven. It should be noted that it is difficult to analyze maternal mortality trends in an individual state. Maternal mortality is relatively rare, so variations due to chance from year to year could be misinterpreted. For example, if a small state had 3 maternal deaths one year and six the following year, an ideologically driven headline might trumpet, “maternal deaths have doubled in state X,” but this change could easily be due to chance.
The CDC cautions against comparing state maternal mortality data, stating “[r]ates based on fewer than 20 deaths are suppressed because of reliability and confidentiality. It is likely that some of the variation in state rates is due to the marked differences in the quality of state maternal mortality data.”[86]
This sentiment was also echoed by researchers outside of the pro-life space in a seminal 2016 paper, “It would be preferable to analyze data individually for each state, however, maternal death is a rare event, and the numbers of cases (396 U.S. deaths in 2000, and 856 in 2014) were not sufficient to support individual state analysis for all but the most populous states (California and Texas).” [87]
For this reason, most comparisons do not focus on individual states but collectively analyze groupings of states. A 2026 JAMA Open Network study examining (n=12,993 deaths out of 22,011,131 births) pregnancy-associated deaths from 2018-2023 found no significant increase in mortality in the fourteen states with “abortion bans” vs. the thirty-seven “non-ban” states (including the District of Columbia).[88] Note that this looks at pregnancy-associated, not pregnancy-related deaths, so causation related to pregnancy was not determined. Unsurprisingly, the pro-abortion journal then invited and published commentary from Amanda Stevenson (author of the first article I discussed) documenting reasons that no effect was seen even though it was still likely to occur.[89]
Another study examined severe maternal morbidity (SMM), rather than mortality, because significant events that cause a woman to become very ill, but ultimately recover (known as “near-miss” events), occur much more commonly than deaths. They examined hospital coding of SMM at less than 24 weeks of gestation and noted no significant changes in the rate of total severe early pregnancy morbidity before and after the Dobbs decision.[90]
Conclusions
It is a fact that maternal mortality in the U.S. has been close to the worst in the developed world for decades, even when abortion was readily available prior to the Dobbs decision, although long-standing data deficiencies limited recognition and discussion of this tragic reality. An honest discussion of this heartbreaking problem requires understanding the definitions and causes of maternal mortality, to determine whether factors that contribute to maternal mortality can expect to become worse in the setting of abortion limitations, and we have addressed this in detail elsewhere.[91]
There are reasons to anticipate that abortion limitations will improve some conditions that may contribute to maternal mortality, such as limiting later more dangerous abortions and exposure to repeat abortions, preventing mental health disorders that may lead to “deaths of despair” in vulnerable women, and possibly preventing future pregnancy complications that may lead to death in a subsequent pregnancy, among other factors. Notably, abortion limitations have not been linked to an increase in maternal mortality in other countries, and some pro-life countries such as Poland and Malta have some of the lowest maternal mortality rates in the world. [92]
It is also a fact that correlation does not equal causation. Factors may be held in common that unite pro-life states and contribute to maternal mortality but that are not necessarily abortion related. Although the researchers of the previously referenced publications undoubtedly understand that the correlation of high maternal mortality in pro-life states does not demonstrate the pro-life laws caused the mortality, the reports are often framed in such a way that this nuanced observation is missed by those who amplify and disseminate the reports’ conclusions to score ideologic points. Although a deeper dive into each of these politically driven reports documents that in some cases they did highlight non-abortion-related contributing factors, the overly simplistic bottom-line conclusions were uncritically picked up by pro-abortion media and disseminated as uncontroversial truths.
We can cautiously point out that the dire predictions of increased maternal mortality due to abortion limitations after Dobbs do not appear to be happening broadly (although quality data lags, awaiting future evaluation). Abortion advocates have focused on pro-life states (especially Texas) with incorrect analyses, ignoring the risk factors that many pro-life states have in common that are unrelated to abortion.
But we must end with a note of warning. Abortion advocates are boldly promoting and selling medically unsupervised mail-order abortion drugs at higher gestational ages and with regimens untested by the FDA, as they prioritize abortion “access” over safety for women and these reckless actions are likely to result in harm to women.[93]
Ingrid Skop, M.D., F.A.C.O.G., is Vice President and Director of Medical Affairs for the Charlotte Lozier Institute.
[1] Maternal Mortality and Maternity Care in the United States Compared to 10 Other Developed Countries, https://www.commonwealthfund.org/publications/issue-briefs/2020/nov/maternal-mortality-maternity-care-us-compared-10-countries.
[2] Texas Heartbeat Act, “SB 8.” 2021, https://capitol.texas.gov/tlodocs/87R/billtext/html/SB00008F.htm.
[3] Stephenson AJ “The pregnancy related mortality impact of a total abortion ban in the U.S.” Demography 2021 Dec 1;58(6):2019-2028. doi: 10.1215/00703370-9585908 https://pubmed.ncbi.nlm.nih.gov/34693444/.
[4] Ingrid Skop, “Handbook of Maternal Mortality: Addressing the U.S. Maternal Mortality Crisis, Looking Beyond Ideology,” Charlotte Lozier Institute, January 6, 2023. https://lozierinstitute.org/handbook-of-maternal-mortality-addressing-the-u-s-maternal-mortality-crisis-looking-beyond-ideology/.
[5] Texas Health and Human Services: Texas Health Data, Maternal Health. https://healthdata.dshs.texas.gov/dashboard/maternal-and-child-health/maternal-health/maternal-health; also personal knowledge as a committee member.
[6] Stephenson 2021.
[7] Ingrid Skop “Fact Check Abortion is 14 times safer than childbirth” Charlotte Lozier Institute https://lozierinstitute.org/fact-check-abortion-is-14-times-safer-than-childbirth/.
[8] Keyfets A, et al. “The impact of hostile abortion legislation on the United States maternal mortality crisis: a call for increased abortion education” Front Public Health 2023 Dec 5;11:1291668. doi: 10.3389/fpubh.2023.129166. https://pmc.ncbi.nlm.nih.gov/articles/PMC10728320/#:~:text=States%20with%20abortion%20bans%20or,reproductive%20age%2C%20and%20greater%20racial.
[9] Ingrid Skop “Response to media allegations that abortion restrictions cause maternal mortality and female suicides.” Charlotte Lozier Institute, https://lozierinstitute.org/response-to-media-allegations-that-abortion-restrictions-cause-maternal-mortality-and-female-suicides/.
[10] Tessa Cox and Ingrid Skop, “Deficiencies affecting U.S. abortion data collection and application”, Charlotte Lozier Institute, https://lozierinstitute.org/fact-sheet-deficiencies-affecting-u-s-abortion-data-collection-and-application/.
[11] Handbook of Maternal Mortality.
[12] Fact Check: Abortion is 14 times Safer Than Childbirth.
[13] Charlotte Lozier Institute, Fact Sheet Abortion and Mental Health, https://lozierinstitute.org/fact-sheet-abortion-and-mental-health/.
[14] Ingrid Skop, “Fact sheet Introduction to maternal mortality,” https://lozierinstitute.org/fact-sheet-introduction-to-maternal-mortality/.
[15] CDC about contraception, https://www.cdc.gov/contraception/about/index.html/.
[16] Ingrid Skop, “Twelve reasons women’s health and maternal mortality will not worsen and may improve in states with abortion limitations,” Charlotte Lozier Institute, https://lozierinstitute.org/twelve-reasons-womens-health-and-maternal-mortality-will-not-worsen-and-may-improve-in-states-with-abortion-limitations/. Phillip B Levine. Sex and Consequences: Abortion, Public Policy, and the Economics of Fertility. https://press.princeton.edu/books/paperback/9780691130453/sex-and-consequences.
[17] Reardon DC, Rafferty KA, Longbons T, “The Effects of Abortion Decision Rightness and Decision Type on Women’s Satisfaction and Mental Health”, Cureus 2023 May 11;15(5):e38882. doi: 10.7759/cureus.38882. https://pubmed.ncbi.nlm.nih.gov/37303450/.
[18] Corinne H. Rocca, Heidi Moseson, Health Gould et al., “Emotions over Five Years After Denial of Abortion in the United States: Contextualizing the Effects of Abortion Denial on Women’s Health and Lives,” Social Science and Medicine 269 (2021), doi:10.1016/j.socscimed.2020.113567.
[19] Stevenson 2021.
[20] Abigail Aiken, Jennifer Starling, James Scott, et al, “Requests for Self-managed Medication Abortion Provided Using Online Telemedicine in 30 US States Before and After the Dobbs v Jackson Women’s Health Organization Decision,” JAMA. 328, no. 17 (2022): 1768-1770. doi:10.1001/jama.2022.18865, https://jamanetwork.com/journals/jama/fullarticle/2797883; Lauren Ralph, Diana Foster, Sarah Raifman, et al. “Prevalence of Self-Managed Abortion Among Women of Reproductive Age in the United States,” JAMA Network Open. 3 no. 12 (2020):e2029245. doi:10.1001/jamanetworkopen.2020.29245.
[21] Response to media allegations that abortion restrictions cause maternal mortality and female suicides.
[22] Paul Linton. “The impact of abortion laws on maternal mortality rates, what is the evidence?” Charlotte Lozier Institute. https://lozierinstitute.org/the-impact-of-abortion-laws-on-maternal-mortality-rates-what-is-the-evidence/.
[23] Nisha Verma, Vinita Goyal, Daniel Grossman, Jamila Perrit, Grace Shih, “Society of Family Planning Interim Clinical Recommendations: Self-managed Abortion,” https://societyfp.org/wp-content/uploads/2022/06/SFP-Interim-Recommendation-Self-managed-abortion-09.08.22.pdf.
[24] Stevenson 2021.
[25] Charlotte Lozier Institute, “Fact Sheet: Risks and Complications of Chemical Abortion,” Charlotte Lozier Institute, August 23, 2023, https://lozierinstitute.org/fact-sheet-risks-and-complications-of-chemical-abortion/; Ingrid Skop, “Induced abortion with misoprostol alone”, Charlotte Lozier Institute, https://lozierinstitute.org/induced-abortion-with-misoprostol-alone-3/.
[26] Nisha Verma, Vinita Goyal, Daniel Grossman, Jamila Perrit, Grace Shih, “Society of Family Planning Interim Clinical Recommendations: Self-managed Abortion,” https://societyfp.org/wp-content/uploads/2022/06/SFP-Interim-Recommendation-Self-managed-abortion-09.08.22.pdf.
[27] “Will Medical Staff be Able to Notice That I am Having an Abortion?”, Safe2Choose, https://safe2choose.org/faq/medical-abortion-faq/during-abortion-with-pills/will-medical-staff-be-able-to-notice-that-i-am-having-an-abortion.
[28] Kavitha Surana, “Afraid to Seek Care Amid Georgia’s Abortion Ban, She Stayed at Home and Died,” ProPublica, September 18, 2024, https://www.propublica.org/article/candi-miller-abortion-ban-death-georgia; Kavitha Surana, “Abortion Bans Have Delayed Emergency Medical Care. In Georgia, Experts Say This Mother’s Death was Preventable”, ProPublica, Sept. 16, 2024.
[29] Eugene Declercq et al., “The U.S. Maternal Health Divide: The Limited Maternal Health Services and Worse Outcomes of States Proposing New Abortion Restrictions.” The Commonwealth Fund 2022. https://www.commonwealthfund.org/publications/issue-briefs/2022/dec/us-maternal-health-divide-limited-services-worse-outcomes.
[30] Planned Parenthood of Southeastern Pa. v. Casey, 505 U.S. 833 (1992). https://supreme.justia.com/cases/federal/us/505/833/.
[31] Ingrid Skop, “Immediate Physical Complications of Induced Abortion”, Charlotte Lozier Institute, December 8, 2022. https://lozierinstitute.org/immediate-physical-complications-of-induced-abortion/.
[32] Comprehensive Health of Planned Parenthood Great Plains, Planned Parenthood Great Rivers-Missouri Plaintiffs, v. the state of Missouri, et al. Defendants.https://statecourtreport.org/sites/default/files/2024-11/planned_parenthood-petition.pdf.
[33] Handbook of Maternal Mortality.
[34] According to the Census Bureau, 12.5 percent of the people nationwide in 2023 lived below the poverty line, however, a number of states that are mapped by the Commonwealth Fund as being “abortion restrictive states” had poverty levels that year that were below the 12.5 national level. These included, for example, Utah (9.0), Idaho (10.1), Arizona (12.4), South Dakota (11.8), North Dakota (9.8), Nebraska (10.5), Kansas (11.2), Iowa (11.3), Missouri (12.0), Wisconsin (10.7), Indiana (12.3), Pennsylvania (12.0), Florida (12.3).
This Census Bureau report shows in Appendix Table 1 the percentage of people in poverty in each state in 2023: https://www2.census.gov/library/publications/2024/demo/acsbr-022.pdf.
This Census Bureau report shows the median household income by state:
https://www2.census.gov/library/publications/2025/demo/acsbr-025.pdf.
[35] Forbes. Les Masterson, “The worst (And Best) States for Healthcare, Ranked.” https://www.forbes.com/advisor/health-insurance/best-worst-states-for-healthcare/
[36] World Population Review. “U.S. States by Race 2026.” https://worldpopulationreview.com/states/by-race
[37] The Commonwealth Fund. David C. Radley, Kristen Kolb, Sara R. Collins, “2025 Scorecard on State Health System Performance: Fragile Progress, Continuing Disparities.” https://www.commonwealthfund.org/publications/scorecard/2025/jun/2025-scorecard-state-health-system-performance
[38] Twelve reasons women’s health and maternal mortality will not worsen and may improve in states with abortion limitations.
[39] HHS who is eligible for Medicaid. https://www.hhs.gov/answers/medicare-and-medicaid/who-is-eligible-for-medicaid/index.html.
[40] Guernsey EK, Hernandez V, Cursio J, et al, “Medicaid Expansion and Severe Maternal Morbidity”, Obstet Gynecol 2026;147:885–91, DOI: 10.1097/AOG.0000000000006303.
[41] Commonwealth Fund. https://www.commonwealthfund.org/publications/issue-briefs/2022/dec/us-maternal-health-divide-limited-services-worse-outcomes.
[42] Gender Equity Policy Institute “Maternal Mortality in the United States After Abortion Bans” April, 2025. https://thegepi.org/maternal-mortality-abortion-bans/; https://www.nbcnews.com/health/womens-health/texas-abortion-ban-deaths-pregnant-women-sb8-analysis-rcna171631.
[43] NBC News, “Texas abortion ban causes deaths in pregnant women,” https://www.nbcnews.com/health/womens-health/texas-abortion-ban-deaths-pregnant-women-sb8-analysis-rcna171631; Texas Standard, “Texas maternal mortality rate rises,” https://texasstandard.org/stories/texas-maternal-mortality-rate-rises-abortion-ban/.
[44] GAO “Maternal Health: Outcomes worsened and disparities persisted during the pandemic.” https://www.gao.gov/assets/730/723432.pdf.
[45] Handbook of Maternal Mortality.
[46] NBC News. A dramatic rise in pregnant women dying in Texas after abortion ban, Erika Edwards, Zinhle Essamuah and Jason Kane, September 20, 2024. https://www.nbcnews.com/health/womens-health/texas-abortion-ban-deaths-pregnant-women-sb8-analysis-rcna171631.
[47] Texas Heartbeat Act.
[48] U.S. states ranking by population 2026. https://worldpopulationreview.com/states.
[49] CDC Fertility rates https://www.cdc.gov/nchs/state-stats/births/fertility-rate.html.
[50] CDC Abortion Surveillance-United States, 2020. https://www.cdc.gov/mmwr/volumes/71/ss/ss7110a1.htm#T1_down.
[51] Guttmacher Institute Abortion facts in California. https://states.guttmacher.org/policies/california/abortion-statistics.
[52] Pew Research “U.S. unauthorized immigrant population,” https://www.pewresearch.org/race-and-ethnicity/2025/08/21/u-s-unauthorized-immigrant-population-reached-a-record-14-million-in-2023/.
[53] Medi-Cal immigrant eligibility, https://www.dhcs.ca.gov/keep-your-Medi-Cal/Pages/Medi-Cal-Immigrant-Eligibility-FAQs.aspx.
[54] “Texas undocumented immigrants health care,” https://www.texastribune.org/2026/03/30/texas-undocumented-immigrants-health-care-hospitals/.
[55] Steven Ross Johnson, “The 10 States With the Highest Poverty Rates: 10. Texas,” US News & World Report, May 7, 2024, https://www.usnews.com/news/best-states/slideshows/us-states-with-the-highest-poverty-rates.
[56] Texas Medical Association, “The Uninsured in Texas,” https://www.texmed.org/uninsured_in_texas/.
[57] Migration Policy Institute, “Profile of the Unauthorized Population: Texas,” https://www.migrationpolicy.org/data/unauthorized-immigrant-population/state/tx.
[58] “Texas Health Data: Chronic Disease,” Texas Department of State Health Services, https://healthdata.dshs.texas.gov/dashboard/surveys-and-profiles/health-facts-profiles/chronic-disease.
[59] “Maternity Care Deserts,” March of Dimes PeriStats, https://www.marchofdimes.org/peristats/data?top=23&lev=1&stop=641®=99&sreg=48&obj=9&slev=4.
[60] Ingrid Skop “Are pro-life laws harming women and children, an examination of claims against Texas,” Charlotte Lozier Institute, https://lozierinstitute.org/are-pro-life-laws-harming-women-and-children-an-examination-of-claims-against-texas/.
[61] KUT, “Like Texas, California once had a maternal mortality crisis, here’s how the state solved it,” https://www.kut.org/health/2018-02-20/like-texas-california-once-had-a-maternal-mortality-crisis-heres-how-the-state-solved-it; KUT, “Here’s how Texas can follow California’s lead in reducing maternal deaths,” https://www.kut.org/health/2018-02-21/heres-how-texas-can-follow-californias-lead-in-reducing-maternal-deaths; KUT, “There’s no success story Texas can follow to stop black mothers from dying,” https://www.kut.org/health/2018-02-22/theres-no-success-story-texas-can-follow-to-stop-black-mothers-from-dying.
[62] Macdorman 2016.
[63] Studnicki J, Fisher JW, Cox T, et al, “Determining the Period Prevalence and Acuity of Emergency Department Visits Following Induced Abortion Mistakenly Identified as Spontaneous Abortion: An Analytic Observational Prospective Cohort Study” Family Medicine and Primary Care: Open Access, 2025 https://www.gavinpublishers.com/article/view/determining-the-period-prevalence-and-acuity-of-emergency-department-visits-following-induced-abortion-mistakenly-identified-as-spontaneous-abortion-an-analytic-observational-prospective-cohort-study.
[64] California Maternity Quality Care Collaborative. https://www.cmqcc.org/toolkits-quality-improvement/all-toolkits.
[65] ACOG Safe motherhood initiative. https://www.acog.org/community/districts-and-sections/district-ii/programs-and-resources/safe-motherhood-initiative; Alliance for Innovation on Maternal Health https://saferbirth.org/patient-safety-bundles/.
[66] Yelp Partners with CHCF to Add Maternity Care Measures to Popular Search and Review Site https://www.chcf.org/resource/yelp-partners-with-chcf-to-add-maternity-care-measures-to-popular-search-and-review-site/.
[67] KUT, “Texas maternal mortality problem is also a data problem, study finds,” https://www.kut.org/health/2018-01-04/texas-maternal-mortality-problem-is-also-a-data-problem-study-finds.
[68] Innovation on Maternal Health (AIM) https://saferbirth.org/.
[69] 2024 “Texas MMMRC-DSHS Joint Biennial Report,” https://www.dshs.texas.gov/sites/default/files/legislative/2024-Reports/MMMRC-DSHS-Joint-Biennial-Report-2024.pdf.
[70] Sabrina Malhi. “Childbirth deadlier for Americans, especially black women, study finds.” June 4, 2024. Washington Post. https://www.washingtonpost.com/health/2024/06/04/us-maternal-mortality-rate-higher-other-countries/
[71] Commonwealth Fund 2022. https://www.commonwealthfund.org/publications/issue-briefs/2022/dec/us-maternal-health-divide-limited-services-worse-outcomes.
[72] “2024 State Scorecard on Women’s Health and Reproductive Care,” The Commonwealth Fund, July 18, 2024. https://www.commonwealthfund.org/publications/scorecard/2024/jul/2024-state-scorecard-womens-health-and-reproductive-care.
[73] Tessa Cox and Ingrid Skop, “Dobbs and medical deserts: Will pro-life laws drive away doctors and lead to hospital closures?” https://lozierinstitute.org/dobbs-and-medical-deserts-will-pro-life-laws-drive-away-doctors-and-lead-to-hospital-closures/.
[74] NRMP Releases Results of the 2026 Main Residency Match for More Than 38,000 Future Residents, https://www.nrmp.org/about/news/2026/03/nrmp-releases-results-of-the-2026-main-residency-match-for-more-than-38000-future-residents/.
[75] Staiger B, Bolotnyy V, Borrero S. “Obstetrician and Gynecologist Physicians’ Practice Locations Before and After the Dobbs Decision.” JAMA Network Open. 2025;8;(4):e251608. doi:10.1001/jamanetworkopen.2025.1608.
[76] Desai S, Jones R, Castle K. “Estimating abortion provision and abortion referrals among United States obstetricians and gynecologists in private practice.” Contraception 2018;97:297-302; Stuhlberg DB, Dude AM, Dahlquist I, Curlin FA. “Abortion provision among practicing obstetrician-gynecologists.” Obstet Gynecol 2011;118(3):609-614.
[77] NPR. As a baby bust hits rural areas, hospital labor and delivery wards are closing down, July 15, 2024. https://www.npr.org/sections/shots-health-news/2024/07/12/nx-s1-5036878/rural-hospitals-labor-delivery-health-care-shortage-birth.
[78] Mary Harned and Ingrid Skop. “Pro-life laws protect mom and baby: Pregnant women’s lives are protected in all states.” Charlotte Lozier Institute, September 11, 2023, https://lozierinstitute.org/pro-life-laws-protect-mom-and-baby-pregnant-womens-lives-are-protected-in-all-states/ ; Ingrid Skop. “Abortion policy allows physicians to intervene to protect a mother’s life.” Charlotte Lozier Institute, May 16, 2023. https://lozierinstitute.org/abortion-policy-allows-physicians-to-intervene-to-protect-a-mothers-life/; and Tessa Cox, Ingrid Skop, Mary Harned. “Fact Sheet: Are Pro-Life State Laws Preventing Pregnant Women from Receiving Emergency Care?” Charlotte Lozier Institute, September 13, 2024. https://lozierinstitute.org/fact-sheet-are-pro-life-state-laws-preventing-pregnant-women-from-receiving-emergency-care/.
[79] In re State, 682 S.W.3d 890, 894 (Tex. 2023), available at https://www.txcourts.gov/media/1458610/230629.pdf.
[80] Kavitha Surana, “Afraid to Seek Care Amid Georgia’s Abortion Ban, She Stayed at Home and Died,” ProPublica, September 18, 2024, https://www.propublica.org/article/candi-miller-abortion-ban-death-georgia; Kavitha Surana, “Abortion Bans Have Delayed Emergency Medical Care. In Georgia, Experts Say This Mother’s Death was Preventable”, ProPublica, Sept. 16, 2024; Lizzie Presser and Kavitha Surana. “A Pregnant Teenager Died After Trying to Get Care in Three Visits to Texas Emergency Rooms,” ProPublica, November 1, 2024, https://www.propublica.org/article/nevaeh-crain-death-texas-abortion-ban-emtala; Cassandra Jaramillo and Kavith Surana, “A Texas Woman Died After the Hospital Said It Would be a ‘Crime’ to Intervene in Her Miscarriage,” ProPublica. October 30, 2024. Available at https://www.propublica.org/article/josseli-barnica-death-miscarriage-texas-abortion-ban; Lizzie Presser and Kavitha Surana, “A Third Woman Died Under Texas’ Abortion Ban. Doctors Are Avoiding D&Cs and Reaching for Riskier Miscarriage Treatments,” ProPublica. November 25, 2024. https://www.propublica.org/article/porsha-ngumezi-miscarriage-death-texas-abortion-ban.
[81] Kavitha Surana and Lizzie Presser. “Texas Medical Board Sanctions Three Doctors for Delayed Care That Led to the Deaths of Two Pregnant Women.” ProPublica, April 17, 2026. https://www.propublica.org/article/tmb-disciplines-doctors-ngumezi-crain-cases.
[82] Maura Quinlan and Paul Linton, “Medically Necessary Abortions After Dobbs: What, if Anything, Has Changed?”, 39 Notre Dame J. L., Ethics & Pub. Pol’y, https://papers.ssrn.com/sol3/papers.cfm?abstract_id=4909792.
[83] Michael New. https://www.liveaction.org/news/jessica-valenti-misleads-dobbs-maternal-infant-mortality; Hoyert DL. Maternal mortality rates in the United States, 2023. NCHS Health E-Stats. 2025. DOI: https://dx.doi.org/10.15620/cdc/174577.
[84] CDC Maternal Mortality 2023 https://www.cdc.gov/nchs/data/hestat/maternal-mortality/2023/fig01.png.
[85] CDC Provisional maternal deaths rates https://www.cdc.gov/nchs/nvss/vsrr/provisional-maternal-deaths-rates.htm.
[86] CDC Maternal mortality 2018-2022 state data https://www.cdc.gov/nchs/maternal-mortality/mmr-2018-2022-state-data.pdf.
[87] MacDorman 2016. (See development of correction factors section.)
[88] HE Abraha. “US Abortion Bans and Pregnancy-Associated Mortality.” JAMA Network Open. https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2847291.
[89] Stevenson AJ, “Invited Commentary: Differences Between State-Level and Nationwide Abortion Bans,” JAMA Network Open. 2026;9(4):e264809. doi:10.1001/jamanetworkopen.2026.4809.
[90] Nourse SE, Gero A, Hunt-Smith TT. “Severe Early Pregnancy Morbidity at a Tertiary Care Referral Center After the Dobbs Decision.” Obstet Gynecol 2026;147:831–4. DOI: 10.1097/AOG.0000000000006163.
[91] Handbook of Maternal Mortality.
[92] Twelve reasons women’s health and maternal mortality will not worsen and may improve in states with abortion limitations; World Population Review: Maternal mortality rates by country. https://worldpopulationreview.com/country-rankings/maternal-mortality-rate-by-country.
[93] Mia Steupert, “An overview of online abortion drug access in post-Dobbs America, https://lozierinstitute.org/an-overview-of-online-abortion-drug-access-in-post-dobbs-america/; Ingrid Skop “Induced abortion with misoprostol alone”, https://lozierinstitute.org/induced-abortion-with-misoprostol-alone-3/; Ingrid Skop “Drug induced abortion after the first trimester,” https://lozierinstitute.org/drug-induced-abortion-after-the-first-trimester/.















{kind=link}